Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
x ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2016
OR
o TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
Commission File Number 001-37368
ADAPTIMMUNE THERAPEUTICS PLC
(Exact name of Registrant as specified in its charter)
|
England and Wales |
|
Not Applicable |
|
(State or other jurisdiction of incorporation or organization) |
|
(I.R.S. Employer Identification No.) |
|
|
|
|
|
101 Park Drive, Milton Park
Abingdon, Oxfordshire OX14 4RY
United Kingdom |
|
(44) 1235 430000 |
|
(Address of principal executive offices) |
|
(Registrant’s telephone number, including area code) |
|
Securities registered pursuant to Section 12(b) of the Act: |
|
Title of each class |
|
Name of exchange on which registered |
|
American Depositary Shares, each representing 6 Ordinary Shares, par value £0.001 per share |
|
The NASDAQ Global Select Market |
|
Securities registered pursuant to Section 12(g) of the Act: |
|
None |
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act.
o Yes x No
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act.
o Yes x No
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days.
x Yes o No
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files).
x Yes o No
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K.
x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer o |
|
Accelerated filer x |
|
|
Non-accelerated filer o (Do not check if a smaller reporting company) |
|
Smaller reporting company o |
|
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act).
o Yes x No
As of June 30, 2016, the last business day of the registrant’s most recently completed second fiscal quarter, the aggregate market value of the registrant’s ordinary shares, par value £0.001 per share, held by non-affiliates was approximately $386,305,126.
As of March 8, 2017 the number of outstanding ordinary shares, par value £0.001 per share, of the Registrant is 424,775,092.
DOCUMENTS INCORPORATED BY REFERENCE
The following documents (or parts thereof) are incorporated by reference into the following parts of this Form 10-K: Certain information required by Part III of this Annual Report on Form 10-K is incorporated from our definitive proxy statement pursuant to Regulation 14A, to be filed with the Commission not later than 120 days after the close of our fiscal year ended December 31, 2016.
Table of Contents
GENERAL INFORMATION
In this Annual Report on Form 10-K (“Annual Report”), “Adaptimmune,” the “Group,” the “Company,” “we,” “us” and “our” refer to Adaptimmune Therapeutics plc and its consolidated subsidiaries, except where the context otherwise requires. “Adaptimmune®” and “SPEAR” are registered trademarks of Adaptimmune.
Information Regarding Forward-Looking Statements
This Annual Report contains forward-looking statements that are based on our current expectations, assumptions, estimates and projections about us and our industry. All statements other than statements of historical fact in this Annual Report are forward-looking statements.
These forward-looking statements are subject to known and unknown risks, uncertainties, assumptions and other factors that could cause our actual results of operations, financial condition, liquidity, performance, prospects, opportunities, achievements or industry results, as well as those of the markets we serve or intend to serve, to differ materially from those expressed in, or suggested by, these forward-looking statements. These forward-looking statements are based on assumptions regarding our present and future business strategies and the environment in which we expect to operate in the future. Important factors that could cause those differences include, but are not limited to:
· our ability to advance our NY-ESO SPEAR T-cells to a point where GlaxoSmithKline, or GSK, exercises the option to license the product and the scope and timing of performance of our ongoing collaboration with GSK;
· our ability to successfully advance our MAGE-A10, MAGE-A4 and AFP SPEAR T-cells through clinical development and the timing within which we can recruit patients in to and treat patients in our clinical trials;
· our ability to further develop our commercial manufacturing process for our SPEAR T-cells, transfer such commercial process to third party contract manufacturers and for such third party contract manufacturers to manufacture SPEAR T-cells to the quality and on the timescales we require;
· the success, cost and timing of our product development activities and clinical trials;
· our ability to successfully advance our SPEAR T-cell technology platform to improve the safety and effectiveness of our existing SPEAR T-cell candidates and to submit Investigational New Drug Applications, or INDs, for new SPEAR T-cell candidates;
· the rate and degree of market acceptance of T-cell therapy generally, and of our SPEAR T-cells;
· government regulation and approval, including, but not limited to, the expected regulatory approval timelines for TCR therapeutic candidates;
· patents, including, any inability to obtain third party licenses, legal challenges thereto or enforcement of patents against us;
· the level of pricing and reimbursement for our SPEAR T-cells, if approved for marketing;
· general economic and business conditions or conditions affecting demand for our SPEAR T-cells in the markets in which we operate, both in the United States and internationally;
· volatility in equity markets in general and in the biopharmaceutical sector in particular;
· fluctuations in the price of materials and bought-in components;
· our relationships with suppliers and other third-party providers;
· increased competition from other companies in the biotechnology and pharmaceutical industries;
· claims for personal injury or death arising from the use of our SPEAR T-cell candidates;
· changes in our business strategy or development plans, and our expected level of capital expenses;
· our ability to attract and retain qualified personnel;
Table of Contents
· regulatory, environmental, legislative and judicial developments including a regulatory requirement to place any clinical trials on hold or to suspend any trials;
· a change in our status as an emerging growth company under the Jumpstart Our Business Start-ups Act of 2012, or JOBS Act”);
· uncertainty about the future relationship between the United Kingdom and the European Union; and
· additional factors that are not known to us at this time.
Additional factors that could cause actual results, financial condition, liquidity, performance, prospects, opportunities, achievements or industry results to differ materially include, but are not limited to, those discussed under “Risk Factors” in Part I, Item 1A in this Annual Report and in our other filings with the Securities and Exchange Commission (the “SEC”). Additional risks that we may currently deem immaterial or that are not presently known to us could also cause the forward-looking events discussed in this Annual Report not to occur. The words “believe,” “may,” “will,” “estimate,” “continue,” “anticipate,” “intend,” “expect” and similar words are intended to identify estimates and forward-looking statements. Estimates and forward-looking statements speak only at the date they were made, and we undertake no obligation to update or to review any estimate and/or forward-looking statement because of new information, future events or other factors. Estimates and forward-looking statements involve risks and uncertainties and are not guarantees of future performance. Our future results may differ materially from those expressed in these estimates and forward-looking statements. In light of the risks and uncertainties described above, the estimates and forward-looking statements discussed in this Annual Report might not occur, and our future results and our performance may differ materially from those expressed in these forward-looking statements due to, inclusive of, but not limited to, the factors mentioned above. Because of these uncertainties, you should not make any investment decision based on these estimates and forward-looking statements.
Table of Contents
Item 1. Business
Overview
We are a clinical-stage biopharmaceutical company committed to developing novel immunotherapies primarily to treat cancer. Our vision is to be a world leader in discovering, developing and commercializing T-cells to transform the treatment of patients with serious diseases. Our comprehensive SPEAR (Specific Peptide Enhanced Affinity Receptor) T-cell platform enables us to identify cancer targets, find and genetically optimize T-cell receptors (“TCRs”), and produce SPEAR T-cells for administration to patients. Unlike certain other autologous immunotherapies our SPEAR T-cells are able to target intracellular and extracellular targets and solid and haematologic tumors.
Our SPEAR T-cell platform is being utilized to maximize both patient and disease indication coverage. First, we are using our platform to identify and validate cancer testis antigens for development of SPEAR T-cells. These antigens have very low expression on normal tissues and are therefore preferred targets for our SPEAR T-cells. However, within a given disease indication, the frequency of expression of these targets may be low, and may not be uniformly expressed in every cell within a tumor. As a result, we are developing multiple SPEAR T-cells to different target antigens within any disease indication to increase treatment potential for any given disease. We have three SPEAR T-cells in clinical trials which are directed to cancer testis antigens, NY-ESO-1, MAGE-A4 and MAGE-A10. The targets to which these SPEAR T-cells are directed are expressed in multiple disease indications including non-small cell lung cancer (“NSCLC”), melanoma, urothelial (bladder) cancers and head and neck cancers, with each of these indications being addressed by at least two of the SPEAR T-cells.
Second, we are developing SPEAR T-cells directed to non-cancer testis antigens which are closely related to a specific disease indication. The first of these SPEAR T-cells is our AFP SPEAR T-cell which is directed to hepatocellular cancer. Further targets closely associated with other cancers are also being validated.
Finally, we are identifying peptides to different Human Leukocyte Antigen (“HLA”) types ensuring that for any given target, for example NY-ESO, MAGE-A10, MAGE-A4 or AFP, we can address patient populations with different HLA types.
We have Phase 1/2 clinical trials ongoing with our NY-ESO and MAGE-A10 SPEAR T-cells and during 2016 opened two additional INDs for our AFP and MAGE A-4 SPEAR T-cells. Our NY-ESO SPEAR T-cell has shown promising initial results in clinical trials with a 50% response rate and 18-month median survival rate reported in synovial sarcoma (a solid tumor) and a 91% response rate at day 100 post autologous stem cell transplant in multiple myeloma. The NY-ESO SPEAR T-cell has shown a promising tolerability profile to date in all clinical trials. Our NY-ESO SPEAR T-cell therapy has breakthrough therapy designation in the United States and has also received orphan drug designation from the U.S. Food and Drug Administration (“FDA”), and European Commission for the treatment of soft tissue sarcoma. The European Medicines Agency (“EMA”) has also granted PRIME regulatory access for the Company’s NY-ESO SPEAR T-cell therapy for the synovial sarcoma indication. We expect further clinical data during 2017.
In addition, we continue to use our SPEAR T-cell platform to identify further target peptides which provide additional coverage for any existing indications or which show high expression in specific cancers. We have identified over 30 intracellular target peptides and have 12 research programs evaluating these peptides.
We also recognize that further development of our SPEAR T-cells will assist in enhancing efficacy and durability of response. We therefore have a number of next generation SPEAR T-cell strategies to further develop and engineer our SPEAR T-cells in addition to the initiation of combination therapy approaches, the first of which is with Merck & Co., Inc’s (“Merck”) KEYTRUDA®. To enable continued innovation and development, we also have collaborations with third parties intended to promote further next generation solutions. These include our collaboration with Universal Cells, Inc. (“Universal Cells”) and our collaboration with Bellicum Pharmaceutical Inc. (“Bellicum”). With Universal Cells, we are looking to develop affinity engineered donor T cells that are universally applicable to all patients. While these “universal cells” would be specific for a given HLA type and target antigen, they would overcome the current limitation of autologous therapies that need to be manufactured specifically for each patient. The enhanced T-cell technology being developed involves selective engineering of cell surface proteins, without the use of nucleases, to develop universal T-cell products. If successful, this will enable us to treat large patient populations with an off-the-shelf product. Our Bellicum collaboration was announced in December 2016 and under the collaboration, we will evaluate Bellicum’s GoTCR technology (inducible MyD88/CD40 co-stimulation, or iMC) with our SPEAR T-cells for the potential to create enhanced T-cell therapeutics.
1
Table of Contents
Our Clinical Product Pipeline
NY-ESO
Our SPEAR T-cell therapy targets the NY-ESO-1 and LAGE-1a cancer antigens which are present in multiple different tumor types. We are conducting Phase 1/2 clinical trials in patients with solid tumours and haematological malignancies including synovial sarcoma, multiple myeloma, NSCLC and ovarian cancer. A pilot trial in myxoid round cell liposarcoma (“MRCLS”) started in December 2016. We are planning to start a pivotal trial in synovial sarcoma, which is dependent on the start and performance of comparability studies. Clinical trials are ongoing in the United States and clinical trial applications have been approved in both Canada and the United Kingdom.
MAGE-A10
Our second SPEAR T-cell therapy, targeting the MAGE-A10 peptide, is currently in clinical trials in the United States. The MAGE-A10 trial in NSCLC was initiated in late 2015. A three tumor trial in urothelial (bladder) cancers, melanoma and head and neck cancers was initiated at The University of Texas MD Anderson Cancer Center (“MD Anderson”) in October 2016 and the trial is currently being initiated at other sites in the United States and Canada. Initial data for our MAGE-A10 clinical trials is anticipated in late 2017 or early 2018.
AFP SPEAR T-cell
An IND for our AFP SPEAR T-cell for the treatment of hepatocellular cancer was opened in 2016. Clinical trial sites in the United States and Europe will be initiated in 2017. Initial data from the AFP clinical trials is anticipated in late 2017 or early 2018.
MAGE-A4 SPEAR T-cell
An IND for our MAGE-A4 SPEAR T-cell program in urothelial (bladder) cancers, melanoma, head and neck cancer, ovarian cancer, NSCLC, esophageal cancer and gastric cancers is now open. Initial data on our MAGE-A4 SPEAR T-cell program is anticipated in late 2017 or early 2018.
The following table summarizes the status of our current clinical trials:
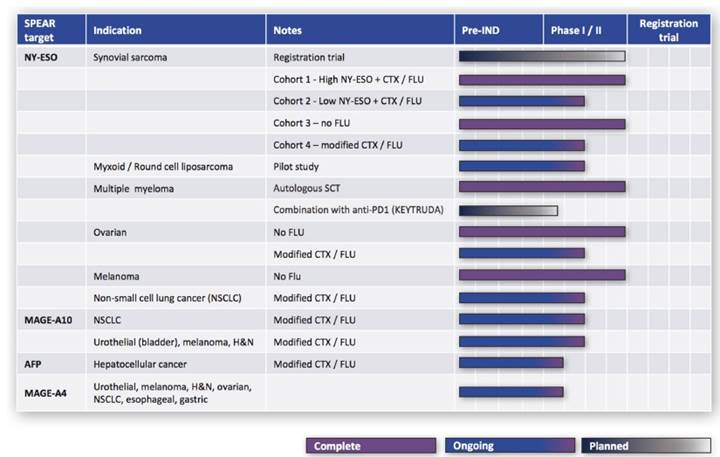
2
Table of Contents
Business Strategy
Our strategic objective is to be a world leader in discovering, developing and commercializing TCR-based T-cell therapies that transform the clinical outcomes of patients with cancer. In order to achieve our objective, we are focused on the following strategies:
Advance our clinical studies for our AFP, MAGE-A10 and MAGE-A4 SPEAR T-cells and advance clinical studies with our NY-ESO SPEAR T-cell beyond the setting of synovial sarcoma where preliminary evidence of efficacy and safety is established. We have four SPEAR T-cells with open INDs covering multiple indications and we plan to advance all four SPEAR T-cells further during 2017 with the aim of providing initial tolerability data for SPEAR T-cells other than our NY-ESO SPEAR T-cell. We are also advancing clinical studies for our NY-ESO SPEAR T-cell in indications other than synovial sarcoma, and clinical trials are already being extended to additional sites within the United States and within Europe. We are also planning to advance into pivotal trials in synovial sarcoma with our NY-ESO SPEAR T-cell. Discussions with the FDA in relation to the planning of that pivotal trial are ongoing.
Continue to use our SPEAR T-cell platform to generate SPEAR T-cells for cancers where existing therapeutic approaches are limited. We intend to continue to generate TCR therapeutic candidates from our fully integrated technology platform, which enables the systematic identification and validation of suitable target peptides, T-cell cloning, engineering of TCRs and preclinical testing processes. The first of our two approaches uses cancer testis antigens and aims to select multiple cancer testis antigens for any given indication to maximize the patient coverage that can be obtained with our SPEAR T-cell products. The second approach relies on the identification of targets which are closely associated with a particular cancer and where the SPEAR T-cells can then be specifically targeted to that cancer.
Continue to understand, further enhance and improve effectiveness and persistence of our SPEAR T-cell therapies. We continue to evaluate and work to understand the mechanism of action of our SPEAR T-cells, in particular the best approaches for enhancing effectiveness and persistence of our SPEAR T-cells. We continue to further develop our TCR therapeutic candidates by exploring the addition of other components in our lentiviral vector, which would be expressed in the SPEAR T-cells alongside the engineered TCR. In addition, we are planning to evaluate the combination of our SPEAR T-cell therapies with other immunotherapy approaches. A combination trial with Merck’s KEYTRUDA® (pembrolizumab) in patients with multiple myeloma is planned to start in 2017.
Optimize and expand our process development and manufacturing capabilities to maintain our leadership position in the TCR space. Our commercial-ready cell manufacturing process (‘cell process 1.5’), has been reviewed by the FDA and the FDA has allowed us to proceed with implementation of cell process 1.5 into our ongoing NY-ESO SPEAR T-cell trials. We continue to optimize the manufacture, supply, associated analytical expertise and quality systems for our SPEAR T-cell therapies to ensure that our manufacturing capability is sufficient for later-stage clinical trials and, potentially, initial commercial supply. We continue to work with third party contract manufacturers in both the United States and Europe to plan for commercial manufacture of our SPEAR T-cells. In addition, during 2016 we completed the shell and core construction for a new state of the art current good manufacturing practice (“cGMP”) manufacturing and office facility and continue to fit-out the facility, which is intended to support the clinical development and initial commercialization of SPEAR T-cells. We are planning to have manufacturing capability towards the end of 2017 and will initially manufacture SPEAR T-cells to support our clinical trials.
Expand our intellectual property portfolio. We intend to continue building on our technology platform, comprising intellectual property, proprietary methods and know-how in the field of TCRs and T-cells. These assets form the foundation for our ability not only to strengthen our product pipeline, but also to defend and expand our position as a leader in the field of T-cell therapies.
Our SPEAR T-cell Therapies
The Immune System and T-cells
The immune system plays an important role in targeting and destroying cancer cells. Specifically, T-cells, which are a type of white blood cell, and their receptors create a natural system that is designed to scan the body for diseased cells. In general, cells process proteins internally and then convert these proteins into peptide fragments which are then presented on the cell surface by a protein complex called the Human Leukocyte Antigen, or HLA. T-cells naturally scan all other cells in the body for the presence of abnormal peptide fragments, such as those generated from infectious agents. Recognition of this peptide-HLA complex takes place through the TCR expressed on the T-cells. Binding of naturally occurring TCRs to cancer targets, however, tends to be very poor because cancer proteins appear very similar to naturally occurring proteins on healthy cells and TCRs that recognise what the body sees as “self-proteins” are eliminated during early human development. Even when TCRs recognize cancer cells expressing novel proteins caused by mutations, elements of the immune system, or the cancer itself often suppress the T-cell response.
3
Table of Contents
Target Identification and Validation
Before developing any engineered T-cell or TCR it is important to identify and validate a suitable target cancer peptide. The target must be expressed primarily only on the cancer cells of interest and with expression in normal non-cancerous tissue only where a risk to the patient would be deemed acceptable. Careful validation and identification of targets is important to ensuring that any engineered TCR is specific to the targeted cancer and does not bind to the same target on non-cancer cells, or that the TCR does not recognize a similar peptide derived from a protein in normal cells. Our target identification platform is focused on three approaches. First, we are using our platform to validate cancer testis antigens. These targets have very low expression on most normal tissues in adults and are therefore preferred targets for our SPEAR T-cells. However, within a given indication, the frequency of expression of these targets may be low, and may not be uniformly expressed in every cell within a tumor. As a result, we are developing multiple SPEAR T-cells to different target peptides in selected disease indications to increase the probability of treating patients with a given disease indication and potentially the ability for re-treatment of patients with a different SPEAR T-cell. We have three SPEAR T-cells in clinical trials which are directed to cancer testis antigens, NY-ESO-1, MAGE-A4 and MAGE-A10. The targets to which these SPEAR T-cells are directed are expressed in multiple disease indications including NSCLC, melanoma, urothelial (bladder) cancers and head and neck cancers, with each of these indications being addressed by at least two of the SPEAR T-cells.
The second type of approach is directed to non-cancer testis antigens which are closely related to a specific disease indication. The first of these SPEAR T-cells is our AFP SPEAR T-cell which is directed to hepatocellular cancer. Further targets closely associated with other cancers are also in development.
Finally, we are identifying targets to different HLA types ensuring that for any given target, we can address patient populations with different HLA types.
Affinity Engineering
Following identification of a suitable target peptide, we identify TCRs that are capable of binding to that target peptide. We then engineer those identified TCRs to enhance and optimize their ability to target and bind to the cancer peptides, thereby enabling a highly targeted immunotherapy. The optimized TCR then undergoes extensive preclinical safety testing prior to administration to patients. Our SPEAR T-cell platform technology enables us to develop a pipeline of targets and TCR therapeutic candidates that we believe may be effective in a variety of cancer types that are unresponsive to currently available and experimental therapies. We have two SPEAR T-cells already in clinical trials (NY-ESO, MAGE-A10), two additional programs with open INDs are planned to enter the clinic in 2017 (AFP and MAGE-A4) and a pipeline of SPEAR T-cells in development.
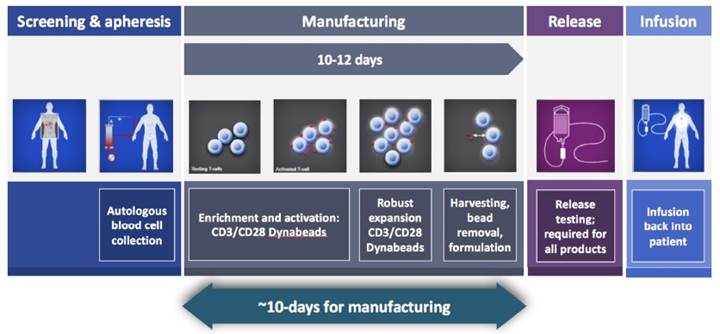
Administration to Patients
The process for treating a patient with an engineered TCR therapeutic candidate involves extracting the patient’s T-cells and then combining the extracted cells with our delivery system containing the gene for our affinity-enhanced TCR, through a process known as transduction. Our delivery system uses a type of self-inactivating (SIN) virus, known as SIN-lentivirus, to transduce the patient’s T-cells and is referred to as a lentiviral vector. The transduced T-cells are then expanded and infused into the patient. When these T-cells encounter a recognized HLA-peptide complex, they multiply and initiate the destruction of the targeted cancer cells. The following diagram summarizes the process for manufacturing and administering our SPEAR T-cells.
4
Table of Contents
Our NY-ESO SPEAR T-cell therapy
Our first SPEAR T-cell targets the NY-ESO-1 and LAGE-1a target peptides and is currently in clinical trials in the United States. Phase 1/2 studies are ongoing in synovial sarcoma, MRCLS, NSCLC and ovarian cancer indications. GSK has an exclusive option over our NY-ESO SPEAR T-cell program. For further details please see “Core Alliances and Collaborations - GSK Collaboration and License Agreement” below.
Our NY-ESO SPEAR T-cell therapy has received orphan drug designation from the FDA and European Commission for the treatment of soft tissue sarcoma. The EMA has also granted PRIME regulatory access for the Company’s NY-ESO SPEAR T-cell therapy for the synovial sarcoma indication, and this product has breakthrough designation in the United States. NY-ESO SPEAR T-cells overall continue to demonstrate a generally acceptable benefit:risk profile to date.
As of January 5, 2017, 61 subjects have received NY-ESO SPEAR T-cells in our sponsored studies. The most common (>15%) adverse events in these subjects considered by investigators to be at least possibly related to our NY-ESO SPEAR T-cells include: fever, diarrhea, fatigue, rash, nausea, anemia, dyspnea, cytokine release syndrome (“CRS”), lymphopenia, leukopenia, cough, ALT increased, AST increased, hypotension, sinus tachycardia, neutropenia, and thrombocytopenia. Adverse events with a severity of grade 3 or higher and considered by investigators to be at least possibly related and occurring in more than one patient include: lymphopenia, leukopenia, anemia, neutropenia, febrile neutropenia, diarrhea, CRS, thrombocytopenia, hypophosphatemia, fever, rash, dyspnea, hypotension, hypoxia, colitis, decreased appetite, dehydration, graft versus host disease, hyponatremia, and musculoskeletal chest pain. There has been one fatal (grade 5) bone marrow failure which was considered related to study treatment by the investigator in the trial. Internal investigations have not identified a mechanism by which the NY-ESO SPEAR T-cells may have caused bone marrow failure. For further details on adverse events please see Part II — Item 1A Risk Factors — “Our SPEAR T-cells may have undesirable side effects or have other properties that could halt their clinical development, prevent regulatory approval, limit their commercial potential or otherwise result in significant negative consequences”.
· Our synovial sarcoma program:
Soft tissue sarcomas can develop from tissues like fat, muscle, nerves, fibrous tissues, blood vessels, or deep skin tissues. There are approximately 50 types of soft tissue sarcomas, including synovial sarcoma, which is a malignant tumor of the soft tissues arising often around joints. Synovial sarcoma is associated with a characteristic chromosomal translocation, and represents about nine percent of all soft tissue sarcomas. This disease is more common in children and young adults, and typically presents at an age ranging from 15 to 40 years. The majority of patients who develop metastatic soft tissue sarcomas are currently incurable, with 75% to 80% of patients not surviving past two to three years. First line therapy typically involves radiotherapy and chemotherapy, as well as surgical resection where possible. There are limited additional treatment options for unresectable, recurrent and metastatic synovial sarcoma, which is nearly always fatal, and systemic therapy is mainly used to provide palliation and slow disease progression.
There are four cohorts in the Phase 1/2 pilot study:
· Cohort 1 (patients with high NY-ESO-1 antigen expression and lymphodepletion with cyclophosphamide and
5
Table of Contents
fludarabine) — enrollment in this first cohort is now complete.
· Cohort 2 (patients with low NY-ESO-1 antigen expression and lymphodepletion with cyclophosphamide and fludarabine) — enrollment continues in this cohort. Indications of a clinical response have also been observed in cohort 2 for one patient out of the 4 evaluable patients treated to date.
· Cohort 3 (patients with high NY-ESO-1 antigen expression and lymphodepletion with cyclophosphamide alone) — only one confirmed response was observed in evaluable patients treated in cohort 3 and as a result, this cohort has now closed. The data from this cohort 3 suggest that fludarabine may be required as part of the pre-conditioning regimen.
· Cohort 4 (patients with high NY-ESO-1 antigen expression and lymphodepletion with a modified (lower) dose of cyclophosphamide and fludarabine) — given the lack of response seen in cohort 3, cohort 4 is open and enrolling patients.
The current synovial sarcoma trials are also being extended to sites outside of the United States with clinical trial applications approved in both the United Kingdom and Canada.
NY-ESO SPEAR T-cells continue to demonstrate a generally acceptable benefit:risk profile to date in synovial sarcoma trials. As of September 30, 2016, our NY-ESO SPEAR T-cells demonstrated a 50% (6/12) response rate in cohort 1 or 60% (6/10) response rate in patients receiving the target cell dose. The median survival rate for patients in cohort 1 is approximately 18 months (80 weeks) as of September 30, 2016.
The diagram below illustrates the best response rate for patients in cohort 1 as of September 30, 2016. Response rate has been determined using Response Evaluating Criteria in Solid Tumors (“RECIST”) 1.1 criteria. The dotted line denotes the level of decrease in target lesion required for a partial response.
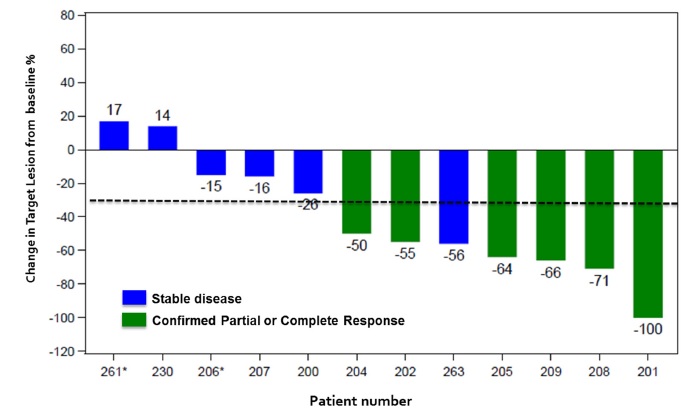

As of January 5, 2017, 24 subjects have received NY-ESO SPEAR T-cells in our synovial sarcoma program. The most common (>30%) adverse events in this trial (all cohorts) considered by investigators to be at least possibly related to our NY-ESO SPEAR T-cells include fever, anemia, lymphopenia, leukopenia, CRS, fatigue, nausea, dyspnea, rash, sinus tachycardia, cough, neutropenia, and thrombocytopenia. Adverse events with severity grade 3 or higher considered by investigators to be at least possibly related and occurring in more than one patient include lymphopenia, leukopenia, anemia, neutropenia, thrombocytopenia, CRS, hypophosphatemia, fever, dyspnea, febrile neutropenia, hypotension, hypoxia, musculoskeletal chest pain, and rash. One patient experienced a fatal bone marrow failure which was considered related to study treatment by the investigator in the trial. Internal investigations have not identified a mechanism by which the NY-ESO SPEAR T-cells may have caused bone marrow failure.
We are in discussions with the FDA in relation to the initiation of a pivotal trial in the synovial sarcoma indication, including discussions relating to trial design and the requirement for comparability testing for use of our manufacturing process. The start of the pivotal trial is dependent on the start and performance of analytical comparability studies between the current and the commercial processes. Should comparability studies be delayed or the results not be acceptable to us or the FDA then the start of the pivotal trial will be delayed.
6
Table of Contents
· Our MRCLS program:
Soft tissue sarcomas can develop from tissues like fat, muscle, nerves, fibrous tissues, blood vessels, or deep skin tissues. There are more than 50 types of soft tissue sarcomas, including MRCLS, which is mostly located in the limbs (most frequently in the thighs). MRCLS is associated with a characteristic chromosomal translocation, and represents about 30 to 35 percent of liposarcomas and 5 to 10 percent of all adult soft tissue sarcomas. MRCLS commonly presents at an age ranging from 35 to 55 years.
A pilot trial in MRCLS is now active at sites in the United States. Initial data from this trial is expected in late 2017 or early 2018 depending on patient recruitment.
This is an open-label pilot study in patients to assess preliminary safety and efficacy in this new indication. Initially, 10 patients will be enrolled. If further characterization of the treatment is required, up to five additional patients may be enrolled. Eligible patients will be HLA-A*02:01, HLA-A*02:05 and/or HLA-A*02:06 with advanced (metastatic or inoperable) MRCLS whose tumor express NY-ESO-1 (defined as >30% of tumor cells that are 2+ or 3+ by immunohistochemistry). Patients will receive preconditioning with fludarabine and cyclophosphamide at the same dose that is being used in cohort 4 of our ongoing synovial sarcoma Phase 1/2 study.
· Our Ovarian program:
Ovarian cancer ranks fifth in cancer deaths among women, accounting for more deaths than any other cancer of the female reproductive system. About 85 to 90 percent of ovarian cancers are cancerous epithelial tumors or epithelial ovarian carcinomas. It is estimated that approximately 22,440 women will receive a new diagnosis of ovarian cancer, and approximately 14,080 women will die of this disease in the United States in 2017. This cancer mainly develops in older women, and approximately half of all ovarian cancers occur in women 63 years of age or older.
The primary trial objective is to determine the safety and tolerability of our NY-ESO TCR therapeutic candidate with chemotherapy preconditioning in patients who have refractory or resistant Stage 3/4 ovarian cancer.
To date, no objective clinical responses have been reported in patients. The initial patients received a preconditioning regimen which consisted of cyclophosphamide alone. The protocol for the ovarian study has now been amended to include a preconditioning regimen which includes both fludarabine and cyclophosphamide. Further data from this trial with the modified preconditioning regimen is expected in late 2017 or early 2018 depending on the rate of patient recruitment.
· Our Melanoma program:
No objective responses have been observed in the four patients treated to date in this trial. As a result, no further patients will be enrolled in the trial. A combination study with immune check point inhibitors (“CPI”) was previously being considered but is no longer being considered given the changes in the underlying standard of care for melanoma patients and the likely difficulty in recruiting patients to such a combination study.
· Our Myeloma program:
Multiple myeloma is a cancer formed by malignancies of plasma cells, which are found in the bone marrow and are an important part of the immune system. It is estimated that approximately 30,280 new cases of multiple myeloma will be diagnosed in the United States in 2017 (17,490 in men and 12,790 in women). Multiple myeloma is characterized by several features, including low blood counts, bone and calcium problems, infections, kidney problems, monoclonal gammopathy, and by the proliferation of malignant plasma cells within bone marrow. The risk of multiple myeloma goes up as people age, and less than one percent of cases are diagnosed in people younger than 35. Most people diagnosed with this cancer are at least 65 years of age.
Enrollment in the myeloma trial (with autologous stem-cell transplantation, or ASCT) was completed in July 2014. The Phase 1/2, open-label, two-site clinical trial in 25 multiple myeloma patients who were eligible for ASCT was open to patients with high risk or relapsed multiple myeloma, who have few remaining treatment options and short life expectancy. Prior to enrollment in the clinical trial, patients had received on average three prior therapies and the trial included six patients that had a prior ASCT. Sixty percent of tumors contained cytogenetic abnormalities that represent negative prognostic indicators. Disease response was assessed in accordance with the International Uniform Response Criteria for myeloma assessment and the additional criteria of nCR which was consistent with the methods employed by the Bone Marrow Transplantation Clinical Trials.
Interim results from this Phase 1/2 clinical trial in multiple myeloma patients were reported in Nature Medicine, published on July 20, 2015. Nature Medicine reported response rates in patients with active disease at the time of transplant, with a 59%
7
Table of Contents
CR/nCR as compared to 24-38% CR/nCR rates at 100 days in other studies treating myeloma with stem cell transplants alone and with stem cell transplants with bortezomib, respectively.
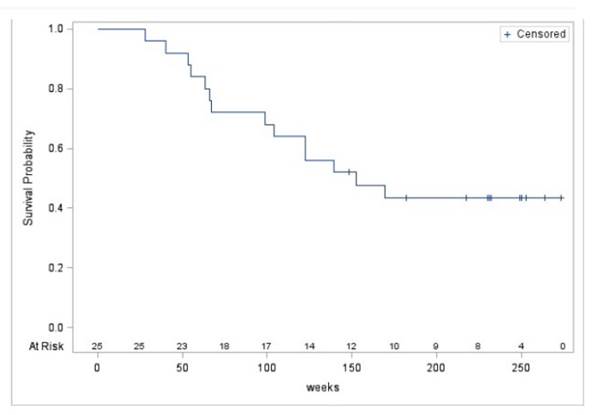
A 91% response rate at day 100 has been previously reported for patients and as of January 27, 2017 there is a median survival rate of approximately three years. Survival data is illustrated in the following Kaplan Meier plot.
As of January 5, 2017, 25 subjects have received NY-ESO SPEAR T-cells in our myeloma transplant program. The most common (>30%) adverse events in this trial considered by investigators to be at least possibly related to our NY-ESO SPEAR T-cells include diarrhea and rash. Adverse events with severity grade 3 or higher considered by investigators to be at least possibly related and occurring in more than one patient include diarrhea, febrile neutropenia, colitis, graft versus host disease, neutropenia and rash.
On October 27, 2016, we announced entry into a clinical trial collaboration agreement for the assessment of our NY-ESO SPEAR T-cell in combination with Merck’s anti-programmed death-1 (“PD-1”) inhibitor, KEYTRUDA® (pembrolizumab), in patients with multiple myeloma. The study will evaluate the safety, pharmacodynamics, and preliminary efficacy of the combination, and is planned for initiation during the second half of 2017.
· NSCLC: A trial in NSCLC opened in 2016. Enrollment has been more challenging than anticipated. Initial data is currently anticipated in late 2017, but availability of data for publication will depend on the number of patients recruited to the trial. The chemotherapy preconditioning regimen has been modified in a protocol amendment to include both fludarabine and cyclophosphamide and the NY-ESO expression requirement has been modified to at least 1+ in >10% of the cells.
Our NY-ESO T-cell therapeutic has also been used in an investigator-initiated clinical program funded by the European Union, the Adoptive Engineered T-cell Targeting to Activate Cancer Killing (“ATTACK 2”) program. The therapy, which is produced under a different manufacturing process than Adaptimmune’s NY-ESO TCR therapy, is being evaluated for the treatment of patients with advanced gastro-esophageal cancer for the first time. Two patients have been treated under this protocol, one of whom passed away 46 days after initial treatment. Enrollment in the trial was temporarily paused pending investigation of the patient fatality, but an independent data monitoring committee has recommended that recruitment can resume following a protocol amendment. The European Union has since terminated funding of the trial due to the delays in trial progression and we are in discussions with the sponsor, the Christie NHS Foundation Trust, in relation to continuation of the trial.
8
Table of Contents
Our MAGE-A10 SPEAR T-cell Therapy
MAGE-A10 is a target peptide expressed in a number of solid tumor cell types, including non-small cell lung cancer (“NSCLC”), urothelial, melanoma and head and neck cancers. Clinical trials are ongoing in the United States in all these tumor types.
· NSCLC: Approximately 80 to 85 percent of all lung cancers are NSCLC, and smoking is by far the leading risk factor. About 40 percent of all NSCLCs are adenocarcinomas. Squamous cell carcinoma is the second most common in the United States and Europe being 25 to 30 percent of NSCLC. Lung cancer is by far the leading cause of cancer death among both men and women, and it is estimated that one out of four cancer deaths are from lung cancer. Lung cancer mainly occurs in older people, and approximately two out of three people diagnosed with lung cancer are 65 or older, while less than two percent are younger than 45.
The initial clinical program in NSCLC is an open label Phase 1 dose escalating study in patients with advanced stage NSCLC expressing the MAGE-A10 antigen. The primary objectives of the study are to assess safety and tolerability of our MAGE-A10 TCR therapeutic candidate in patients. Secondary objectives include the assessment of efficacy and durability of persistence. Enrollment of patients into this program has been challenging. Initial data is expected in late 2017 or early 2018 depending on patient enrollment.
· 3-tumor trial - A three tumor trial in urothelial, melanoma and head and neck cancers received RAC (the NIH Recombinant DNA Advisory Committee) approval in May 2016. The first trial site, MD Anderson, is now initiated and the trial is currently being initiated at other sites in the United States and Canada. This is a Phase I, open-label, modified 3+3 dose escalation study of autologous T-cells genetically engineered with an affinity optimized MAGE-A10 T-cell receptor in HLAA*0201 and HLA-A*0206 positive patients with inoperable or metastatic urothelial cancer (transitional cell cancer of the bladder, ureter or renal pelvis), melanoma, or squamous cell carcinoma of the head and neck expressing the MAGE-A10 antigen.
· Urothelial: Urothelial carcinoma is the most common type of bladder cancer. These cancers mainly start in the urothelial cells that line the inside of the bladder or other parts of the urinary tract. Bladder cancer accounts for approximately five percent of all new cancers in the United States, and is the fourth most common cancer in men. Men are about three to four times more likely to get bladder cancer than women. It is estimated that 79,030 new cases of bladder cancer will be diagnosed (about 60,490 in men and 18,540 in women), and about 16,870 deaths from bladder cancer will occur (about 12,240 in men and 4,630 in women) in the United States in 2017. Bladder cancer occurs mainly in older people, and approximately 9 out of 10 people with this cancer are over the age of 55.
· Melanoma: Melanoma is a cancer that begins in specific skin cells called melanocytes, and exposure to ultraviolet rays is a major risk factor for most melanomas. It is estimated that approximately 87,110 new melanomas will be diagnosed (about 52,170 in men and 34,940 in women), and about 9,730 people are expected to die of melanoma (about 6,380 men and 3,350 women) in the United States in 2017. The risk of melanoma increases as people age, and the average age at diagnosis is 63 years. However, melanoma is not uncommon among those younger than 30, and it is one of the most common cancers in young adults (especially young women).
· Head and Neck: Cancers of the head and neck, which include cancers of the oral cavity, larynx, pharynx, salivary glands, and nose/nasal passages, account for approximately three percent of all malignancies in the United States. At least 75 percent of head and neck cancers are caused by tobacco and alcohol use. Infection with cancer-causing types of human papillomavirus (“HPV”) is also a risk factor for some types of head and neck cancers. In recent years, there has been a drop in the incidence of head and neck cancers caused by tobacco and alcohol, and a rise in the incidence of head and neck cancers caused by HPV.
Our AFP SPEAR T-cell Therapy
AFP is a target peptide associated with hepatocellular carcinoma. Hepatocellular carcinoma is the most common type of liver cancer in adults. Many patients who develop liver cancer have long-standing cirrhosis (scar tissue formation from liver cell damage), and early detection can be difficult because signs and symptoms often do not appear until later stages. It is estimated that approximately 40,710 new cases of liver cancer will be diagnosed (about 29,200 in men and 11,510 in women) and about 28,920 people will die from this disease (about 19,610 men and 9,310 women) in the United States in 2017.
An IND for a clinical trial of our AFP SPEAR T-cell in hepatocellular cancer was opened in 2016 and we anticipate site initiation in the first half of 2017. Enrollment is dependent on the availability of the vector used to manufacture our AFP SPEAR T-cell. The Phase 1 clinical trial will include a dose escalation and expansion of a tolerable dose to explore initial evidence of anti-tumor activity. The trial will also include evaluation of two pre-treatment regimens, one with fludarabine and one without fludarabine.
9
Table of Contents
Our MAGE-A4 SPEAR T-cell Therapy
The FDA has accepted the Company’s IND application for autologous genetically modified T-cells expressing an affinity optimized TCR specific for MAGE-A4 in patients with multiple malignant solid tumors. The IND is now active and we are actively working with sites in the United States to get the study started as soon as possible in 2017.
Under this IND, Adaptimmune will initiate a Phase 1, open-label, modified 3+3 dose escalation study of autologous T-cells genetically engineered with an affinity optimized MAGE-A4 TCR in HLA*02 positive patients with inoperable locally advanced or metastatic melanoma, and urothelial, head and neck, ovarian, non-small cell lung, esophageal, and gastric cancers expressing the MAGE-A4 target peptides. Patients will receive preconditioning with modified fludarabine and cyclophosphamide as used in the Company’s ongoing synovial sarcoma study. This multi-tumor study will enroll up to 32 patients. The trial will also include dose escalation in initial patients.
Initial data is anticipated in late 2017 or early 2018.
Next Generation Technology Platform Development
Next Generation Therapeutics
We believe that there is also further room to enhance the potency and durability of our SPEAR T-cells, for instance by adding further active proteins into the lentiviral delivery system. These enhancements are designed to result in generation 2 SPEAR T-cells for future clinical programs. We have multiple development programs ongoing which are researching different modifications to our SPEAR T-cells. For example, we have an active development program for a ‘dnTGFBRII’ SPEAR T-cell. This next generation SPEAR T-cell is designed to block immune suppression by TGFB in certain tumor microenvironments, thereby enhancing the activity and duration of response seen with our SPEAR T-cells within those environments. We are also considering CD8 constructs where the aim is to promote the antigen spread, anti-tumor memory and tumor inflammation seen with our SPEAR T-cells. We are currently in the process of planning INDs for at least one next generation SPEAR T-cell for 2018.
Manufacturing Improvements
In parallel with our ongoing clinical programs and underlying target peptide identification work, we are improving the processes for manufacture of our lentiviral vector and SPEAR T-cells. Our goal is to achieve a more consistent and efficient manufacturing process and ultimately to reduce the cost of supply.
We have made a number of changes to our current SPEAR T-cell manufacturing process. In particular, we are now streamlining some of the manual steps in the process by simplifying the initial T-cell selection through increased use of the antibody-bound magnetic Dynabeads® CD3/CD28. We are also introducing cryopreservation steps which make the logistics of administering our SPEAR T-cells more flexible for patients and will also facilitate treatment of patients outside the United States. Expansion and harvest of the SPEAR T-cells is now serum-free after initial culture preparation and is being further optimized. A data package for this amended process (‘cell process 1.5’) was submitted to the FDA during 2016 and the FDA has allowed us to proceed with implementation of this cell process 1.5 into our ongoing NY-ESO SPEAR T-cell trials. Finally, we are also working towards automation of at least certain parts of the manufacturing process.
For the vector supply, we are developing and evaluating alternative approaches to increase volume and continuity of supply while at the same time decreasing the cost of the vector supply.
Additionally, in connection with our SPEAR T-cells, we are also working with third-party contractors to develop companion diagnostics for screening of patient tumors for the presence of target peptides.
Core Alliances and Collaborations
GSK Collaboration and License Agreement
We entered into a strategic collaboration and license agreement with GSK in May 2014 (the “GSK Collaboration and License Agreement”) regarding the development, manufacture and commercialization of TCR therapeutic candidates. The collaboration is for up to five programs, the first being the NY-ESO SPEAR T-cell program.
Under the GSK Collaboration and License Agreement, the NY-ESO SPEAR T-cell program and associated manufacturing optimization work will be conducted by us in collaboration with GSK. GSK has an option to obtain an exclusive worldwide license to the NY-ESO therapeutic candidate program, exercisable during the performance of the program and up to specified time periods after we have delivered a Phase 1/2 data package for the program to GSK. If the option is exercised after delivery of the Phase 1/2 data package, GSK will assume full responsibility for the NY-ESO SPEAR T-cell program. In February 2016, the GSK Collaboration and
10
Table of Contents
License Agreement was expanded to accelerate the development of the NY-ESO SPEAR T-cells towards pivotal trials in synovial sarcoma, as well as the exploration of development of NY-ESO SPEAR T-cells in MRCLS. The amendment also provides the opportunity for up to eight combination studies using NY-ESO SPEAR T-cells. As the program progresses, additional amendments to the scope and timing of the NY-ESO development plan may be agreed with GSK.
A second target, PRAME, has also now been nominated by GSK under the GSK Collaboration and License Agreement. As a result of the nomination, Adaptimmune will be responsible for taking the PRAME SPEAR T-cell program through preclinical testing and up to IND filing. GSK is responsible for the IND filing itself. GSK has an exclusive option over the program. Under the terms of the GSK Collaboration and License Agreement, the potential development milestones eligible related to the PRAME program could amount to approximately $300 million, if GSK exercises its option and successfully develops this target in more than one indication and more than one HLA type. Adaptimmune would also receive tiered sales milestones and mid-single to low double-digit royalties on worldwide net sales.
Three other targets may be nominated by GSK at specified times under the GSK Collaboration and License Agreement, excluding any research programs already in progress. Upon nomination by GSK of any of these three additional targets, we will grant to GSK an exclusive option on each target, which can be exercised up to four months after approval of an IND in relation to a TCR therapeutic candidate directed against the nominated target. Nomination also triggers the start of a collaboration program to develop the relevant TCR therapeutic candidate directed to the nominated target peptide.
Following exercise of any option (including the options for the NY-ESO SPEAR T-cell and PRAME SPEAR T-cell programs), we will grant to GSK an exclusive worldwide license under intellectual property rights specific to the SPEAR T-cell developed under the relevant collaboration programs. GSK will, at its own expense, be fully responsible for all further development and commercialization of the relevant T-cell candidates. Under the NY-ESO SPEAR T-cell program, in the event of early exercise of the option, we will, unless otherwise agreed with GSK, have a continuing obligation to complete any work outstanding under the agreed development plan for the NY-ESO SPEAR T-cell program. The licenses do not include a right for GSK to develop alternative affinity-enhanced TCRs using our intellectual property rights or to develop other TCR therapeutic candidates directed to different target peptides. Under the agreement, we are also prohibited from independently developing or commercializing T-cell therapeutics directed at the targets subject to outstanding options granted to GSK.
Under the GSK Collaboration and License Agreement, we received an upfront payment of $42.1 million in June 2014 and are entitled to various milestone payments based on the achievement of specified development and commercialization milestones. As of December 31, 2016, we had achieved development milestones of $39.0 million.
In addition to the development milestones, we are entitled to royalties from GSK on all GSK sales of T-cell products licensed under the agreement, varying between a mid-single-digit percentage and a low-double-digit percentage of net sales, subject to certain agreed reductions, dependent on the cumulative annual net sales for each calendar year. Royalties are payable while there is a jointly owned or solely owned valid patent claim covering the TCR therapeutic in the country in which the relevant TCR therapeutic is being sold and, in each case, for a minimum of 10 years from first commercial sale of the relevant TCR therapeutic. Sales milestones also apply once any TCR therapeutic covered by the GSK Collaboration and License Agreement is on the market.
The GSK Collaboration and License Agreement is effective until all payment obligations expire, including any ongoing royalty payments due in relation to GSK’s sale of any covered TCR therapeutic candidates. The agreement can also be terminated on a collaboration program-by-collaboration program basis by GSK for lack of feasibility or inability to meet certain agreed requirements. Both parties have rights to terminate the agreement for material breach upon 60 days’ written notice or immediately upon insolvency of the other party. GSK has additional rights to terminate either the agreement or any specific license or collaboration program upon 60 days’ written notice to us. Additional payments may be due to us as a result of such termination, and where we continue any development of any TCR therapeutic candidate resulting from a terminated collaboration program, depending on the stage of development, royalties may be payable to GSK at a mid-single-digit percentage rate of net sales. We also have rights to terminate any license where GSK ceases development or withdraws any licensed TCR therapeutic in specified circumstances.
Details of the relationship are also set out in “Risk Factors — Risks Related to Our Reliance Upon Third Parties — We rely heavily on GSK for our NY-ESO TCR therapeutic candidate clinical program, which may also affect other SPEAR T-cell programs”.
MD Anderson Strategic Alliance
On September 26, 2016, we announced that we had entered into a multi-year strategic alliance with MD Anderson designed to expedite the development of T-cell therapies for multiple types of cancer. The Company and MD Anderson will collaborate in a number of studies including clinical and preclinical development of Adaptimmune’s SPEAR T-cell therapies targeting NY-ESO, MAGE-A10 and future clinical stage first and second generation SPEAR T-cell therapies such as MAGE-A4 across a number of cancers, including bladder, lung, ovarian, head and neck, melanoma, sarcoma, esophageal and gastric cancers. The Company will make payments to MD Anderson as certain milestones are achieved and these costs will be expensed to research and development as MD Anderson renders the services.
Under the terms of the alliance agreement, Adaptimmune will sponsor a number of clinical and preclinical studies. Adaptimmune has committed funding of at least US $19,644,000 to fund studies under the alliance agreement. Payment of this funding is contingent on mutual agreement to study orders, in order for any study to be included under the alliance, and the performance of set milestones by MD Anderson.
11
Table of Contents
The alliance and the performance of the various studies will be overseen by a joint steering committee. Decisions of the joint steering committee require unanimity, with one vote being given to each party to the agreement. MD Anderson will supply the required personnel, facilities and equipment for performance of the agreed studies and Adaptimmune will, where applicable, supply the SPEAR T-cell therapy for patient administration.
We will own all results and data arising from the performance of the alliance studies, save for original source documents and patient records. MD Anderson retains the right to use such results and data for its internal research, academic, and patient care purposes. Certain intellectual property rights arising under the alliance will be owned by the Company, with others being owned by the party or parties creating such intellectual property rights. MD Anderson grants to the Company a non-exclusive, worldwide, irrevocable royalty-free license to any arising intellectual property rights in which MD Anderson has an ownership interest, for any purpose. Such license includes an unrestricted right to sublicense through multiple tiers. MD Anderson also grants the Company an exclusive option to negotiate an exclusive (subject to MD Anderson’s perpetual, irrevocable, no-cost right to use such invention for non-commercial internal research, academic and patient care purposes), royalty-bearing license to any arising intellectual property rights in which MD Anderson has an ownership interest. In turn, the Company grants to MD Anderson a limited, perpetual, irrevocable, non-exclusive, royalty-free license to any arising intellectual property rights in which it has an ownership interest for internal non-commercial research, academic and patient care purposes.
The alliance agreement may be terminated by either party for material breach by the other party. Individual studies may be terminated inter alia for material breach, health and safety concerns or where the institutional review board (“IRB”), the review board at the clinical site with oversight of the clinical study, requests termination of any study. Where any legal or regulatory authorization is finally withdrawn or terminated, the relevant study will also terminate automatically.
Merck Combination Agreement
On October 27, 2016, we entered into a clinical trial collaboration agreement with Merck (known as MSD outside the United States and Canada), for the assessment of our NY-ESO SPEAR T-cell therapy in combination with Merck’s PD-1 inhibitor, KEYTRUDA® (pembrolizumab), in patients with multiple myeloma. The study will evaluate the safety, pharmacokinetics, pharmacodynamics, and preliminary efficacy of the combination, and is planned for initiation in the first half of 2017.
Our NY-ESO SPEAR T-cell therapy has previously been evaluated in multiple myeloma in a single agent Phase 1/2 trial in which 20 out of 22 patients (91%) experienced a response at day 100 post autologous stem cell transplant. KEYTRUDA® is a humanized monoclonal antibody that works by increasing the ability of the body’s immune system to help detect and fight tumor cells. KEYTRUDA® blocks the interaction between PD-1 and its ligands, PD-L1 and PD-L2, thereby activating T lymphocytes which may affect both tumor cells and healthy cells. Blocking this interaction is reported to enable T-cell activation and potentiates antitumor activity.
We believe there is preclinical evidence to support the view that the combination of NY-ESO SPEAR T-cell therapy and anti-PD-1 therapy may lead to meaningful anti-tumor activity. We are planning to evaluate our therapy alone and in combination with KEYTRUDA® in a randomized trial of patients with multiple myeloma who are refractory or have relapsed with standard therapy.
Under the terms of the agreement, each of Merck and the Company will manufacture and supply its relevant compound for use in the combination study. Adaptimmune will act as the sponsor for the combination study. Each party will be responsible for its own internal costs associated with the agreement and Adaptimmune will be responsible for the other costs of the combination study. Coordination of the activities under the agreement is via a joint development committee, which comprises an equal number of members from each party. Intellectual property rights under the agreement will, depending on the nature of such rights, be owned solely by either party or jointly. The agreement will last until the earlier of delivery of the final study report or study completion. Either party may terminate the agreement for material breach, patient safety, regulatory action preventing supply of compound or withdrawal of regulatory approval for one of the combination study compounds. Merck may also terminate the agreement where it believes its compound is being used in an unsafe manner.
Universal Cells Research, Collaboration and License Agreement
On November 25, 2015, we entered into a Research, Collaboration and License Agreement relating to gene editing and HLA-engineering technology with Universal Cells. The Company paid an upfront license and start-up fee of $2.5 million to Universal Cells in November 2015 and a milestone payment of $3.0 million in February 2016. Further milestone payments of up to $44 million are payable if certain development and product milestones are achieved. Universal Cells would also receive a profit-share payment for the first product, and royalties on sales of other products utilizing its technology. The upfront and start-up fee was expensed to research and development when incurred.
Under the agreement, the companies have mutually agreed to a development plan for the development of affinity-enhanced donor T-cells that are universally applicable. The enhanced T-cell technology being developed involves selective engineering of cell surface proteins, without the use of nucleases, to develop universal T-cell products. The development plan is split into a series of
12
Table of Contents
phases which can be varied as the project progresses and dependent on the output of earlier phases. The development plan is overseen by a joint steering committee consisting of equal members from each party.
Under the terms of the agreement, Universal Cells grants to Adaptimmune an exclusive, sub-licenseable, worldwide right and license in the field of T-cell immunotherapy, with the right to grant sublicences, under certain intellectual property rights of Universal Cells. The agreement also includes the sub-license of certain intellectual property rights owned by the University of Washington. Adaptimmune grants to Universal Cells a non-exclusive license under its intellectual property rights to the extent required for the performance of the development program.
The agreement will expire on the last to expire of any of the Universal Cells licensed intellectual property, unless terminated earlier for material breach or insolvency. Adaptimmune also has a right to terminate the agreement on provision of written notice where it has safety concerns, does not wish to proceed to the next phase of development or in the event of a change of control.
Bellicum Pharmaceuticals Inc, Co-Development and Co-Commercialization Agreement
On December 16, 2016, we entered into a Co-Development and Co-Commercialization Agreement with Bellicum in order to facilitate a staged collaboration to evaluate, develop and commercialize next generation T-cell therapies.
Under the agreement, we will evaluate Bellicum’s GoTCR technology (inducible MyD88/CD40 co-stimulation, or iMC) with our SPEAR T-cells for the potential to create enhanced T-cell therapeutics. Depending on results of the initial preclinical proof-of-concept phase, we may progress to a two-target co-development and co-commercialization phase. To the extent necessary, and in furtherance of the parties’ proof-of-concept and co-development efforts, the parties granted each other a royalty-free, non-transferable, non-exclusive license covering their respective technologies for purposes of facilitating such proof—of-concept and co-development efforts. In addition, as to covered therapies developed under the agreement, the parties granted each other a reciprocal exclusive license for the commercialization of such therapies.
With respect to any joint commercialization of a covered therapy, the parties agreed to negotiate in good faith the commercially reasonable terms of a co-commercialization agreement. The parties also agreed that any such agreement shall provide for, among other things, equal sharing of the costs of any such joint commercialization and the calculation of profit shares as set forth in the agreement.
The agreement will expire on a country-by-country basis once the parties cease commercialization of the T-cell therapies covered by the agreement, unless earlier terminated by either party for material breach, non-performance or cessation of development, bankruptcy/insolvency, or failure to progress to co-development phase.
Intellectual Property
We actively seek to protect the intellectual property and proprietary technology that we believe is important to our business, including seeking, maintaining, enforcing and defending patent rights for our SPEAR T-cells and processes, whether developed internally or licensed from third parties. Our success will depend on our ability to obtain and maintain patent and other protection including data/market exclusivity for our SPEAR T-cells and SPEAR platform technology, preserve the confidentiality of our know-how and operate without infringing the valid and enforceable patents and proprietary rights of third parties. See “Risk Factors—Risks Related to Our Intellectual Property.”
Our policy is to seek to protect our proprietary position generally by filing an initial priority filing at the U.K. Intellectual Property Office (“UKIPO”) and the U.S. Patent Trademark Office (“USPTO”). This is followed by the filing of a patent application under the Patent Co-operation Treaty claiming priority from the initial application(s) and then application for patent grant in, for example, the United States, Europe (including major European territories), Japan, Australia, New Zealand, India and Canada. In each case, we determine the strategy and territories required after discussion with our patent professionals to ensure that we obtain relevant coverage in territories that are commercially important to us and our TCR therapeutic candidates. We will additionally rely on data exclusivity, market exclusivity and patent term extensions when available, including as relevant exclusivity through orphan or pediatric drug designation. We also rely on trade secrets and know-how relating to our underlying platform technology, manufacturing processes and SPEAR T-cells. Prior to making any decision on filing any patent application, we consider with our patent professionals whether patent protection is the most sensible strategy for protecting the invention concerned or whether the invention should be maintained as confidential.
As of December 31, 2016 we owned or jointly owned approximately 173 granted patents (of which 18 are U.S.-issued patents) and 69 pending patent applications (of which 7 are U.S. National patent applications). These patents and patent applications include claims directed to our SPEAR T-cells, our platform technology used to identify and generate engineered TCR therapeutic candidates and our manufacturing and process technology.
13
Table of Contents
Product Patents
NY-ESO - We own granted patents covering the composition of matter of our NY-ESO SPEAR T-cell. The patent claims are directed to the NY-ESO SPEAR TCR and in particular the amino acid substitutions required for such engineered TCR therapeutic candidate. The patent has been granted in major territories including Australia, Europe (Switzerland, Germany, Denmark, France, United Kingdom, Ireland and the Netherlands), New Zealand, Japan and the United States. These granted patents are expected to expire in May 2025.
MAGE-A10 - We own patent applications covering the composition of matter of our MAGE-A10 TCR therapeutic candidate. The patent application claims are directed to the engineered TCR therapeutic candidate and in particular the amino acid substitutions required for such engineered TCR therapeutic candidate. The patent applications have been filed with the UKIPO and with the USPTO and we are in the process of filing national applications in all the commercially relevant territories.
AFP — We own patent applications covering the composition of matter of our AFP therapeutic candidate. As with our NY-ESO and MAGE-A10 TCR therapeutic candidates, the patent application claims are directed to the engineered TCR therapeutic candidate and in particular the amino acid substitutions required for such engineered TCR therapeutic candidate. An initial priority patent application was filed in the UKIPO and a patent application under the applicable Patent Co-operation Treaty has since been filed claiming priority from that U.K. patent application. National applications have been filed in all commercially relevant territories.
MAGE-A4 - We own three patent applications covering the composition of matter of our MAGE-A4 therapeutic candidate and other related TCRs. As with our NY-ESO and MAGE-A10 TCR therapeutic candidates, the patent application claims are directed to the engineered TCR therapeutic candidate and in particular the amino acid substitutions required for such engineered TCR therapeutic candidate. The initial priority patent applications were filed in the UKIPO.
Platform Technology
We jointly own a number of platform technology patents and patent applications. These are jointly owned with Immunocore Limited (“Immunocore”) and are directed to certain aspects of the process that we use to engineer our SPEAR TCRs. For example, patents directed to the di-sulphide bond stabilization technique required to solubilize TCRs for isolation, characterization and validation have been issued in major territories including Australia, Canada, China, major European territories (including the United Kingdom, France, Germany, Spain and Italy), India, Hong Kong, Japan, the United States and South Africa and are expected to expire beginning in 2022. Patents have also been granted in relation to our phage display approach for TCRs and are expected to expire beginning in 2023. The priority patent application was filed in 2002 and patents are now granted in the United States, Australia, Canada, China, major European territories (including the United Kingdom, France, Germany, Spain and Italy), Japan, South Africa, India, Norway and New Zealand. Other examples include an issued patent directed to a method for increasing the affinity of given TCRs to a target peptide (expected to expire in 2025) and patent applications directed to decreasing off-target reactivity and selection for the affinity-enhanced TCRs.
Novel targets
We have filed 29 patent applications under the Patent Cooperation Treaty which cover peptides expressed on the tumor cell surface and the TCRs which recognize them. The applications as filed cover 872 peptides from 63 different target proteins.
TCR libraries
We have filed 10 patent applications which cover large libraries of TCR genes which we have generated and the method of their generation: these act as proprietary sources for screening for TCRs which are the starting points for engineering into clinical candidates.
Manufacturing Process Patents and Patent Applications
We also have know-how and patent applications that we own which relate to the manufacture of our SPEAR T-cells. For example, we have filed patent applications in the major territories, which claim priority from initial priority patent applications filed at the USPTO and UKIPO, which are directed to a particular modification to the lentiviral vector technology. We believe this modification enhances the safety profile of the lentiviral vector technology.
Next Generation Approaches
We have recently filed a priority generating patent application in relation to a gene which prevents our cytotoxic T-cells from being inhibited by the immunosuppressive tumor microenvironment. This is relevant to all of our products in solid tumor
14
Table of Contents
indications and protects one of the next generation SPEAR T-cell products under development. Further next generation patent applications are expected to be filed shortly.
Exclusive License for Bead Products
In December 2012, we entered into two agreements, a license and a sub-license, with ThermoFisher Scientific Inc. (“ThermoFisher”). The license agreement grants us a field-based exclusive license under certain intellectual property rights owned or controlled by ThermoFisher in relation to the methods of use of the ThermoFisher Scientific Dynabeads® CD3/CD28 technology to isolate, activate and expand T cells and enable transfection of the T cells with any TCR genes to manufacture our licensed products and use and sell those TCR products to treat cancer, infectious disease and/or autoimmune disease. The licensed field relates to the ex-vivo activation and expansion of human T cells containing engineered TCRs for use as a therapy for treating cancer, infectious disease and/or autoimmune disease and where the therapy comprises the steps of (a) removing a sample containing T cells from a patient; (b) isolating T cells from that sample using the ThermoFisher bead product or similar magnetic beads; (c) transfecting those isolated T cells with a gene or genes encoding engineered TCRs of known antigen specificity; (d) activating and expanding the population of those engineered T cells using the ThermoFisher bead product or similar magnetic beads; and (e) introducing the expanded, engineered T cells back into the same patient. The license is not sub-licensable, but we are able to sub-contract manufacture of the licensed products to our contract manufacturing organizations. Our sub-licensees have access to the required license directly from ThermoFisher under the above-described intellectual property rights on terms equivalent to those we have obtained from ThermoFisher in relation to our partnered licensed products.
We have granted an option under the license agreement to ThermoFisher to take an exclusive license under any improvements made by or for, or controlled by, us to the ThermoFisher patented technology to the extent any such improvements are dominated by the patent rights licensed to us. Any license will be outside of the exclusive field we have been granted, namely engineered T-cell therapy.
Under the license agreement, we have to demonstrate reasonable commercial efforts to carry out development and commercialization of the licensed products and we are required to make certain expenditures for research and development relating to the commercialization of the licensed products. This obligation is deemed satisfied upon first commercial sale of a licensed product. We have certain payment obligations under the license agreement including an upfront license fee of $335,000, which has already been paid, minimum annual royalty (in the low tens of thousands of U.S. dollars prior to licensed product approval and thereafter at a level of 50% of running royalties in the previous year), milestone payments (payable for each licensed product on achievement of certain development and commercialization milestones per licensed product) and a low single-digit running royalty payable on the net selling price of each licensed product. The license agreement will last until the expiration of the latest to expire of the licensed patent rights. The license agreement can be terminated before the end of its term by mutual agreement, by ThermoFisher on the occurrence of certain events (failure to use reasonable commercial efforts, willful making of a false statement of a material fact, breach of antitrust laws or other laws, material breach of the agreement, payment default or if we have challenged the validity or enforceability of any of the licensed patents). The license may also be terminated in the event of insolvency by either party.
We also have a field-based exclusive sub-license under certain other patents which cover the method of use of the Dynabeads® CD3/CD28 and are controlled by ThermoFisher under a head-license from the University of Michigan, the U.S. Navy and the Dana-Farber Cancer Institute. The sub-license has the same relevant exclusivity scope and field-based restrictions and many of the terms are equivalent to those set out in the main license agreement with ThermoFisher, including the same requirement to demonstrate reasonable commercial efforts to carry out development and commercialization of the licensed products as in the main license agreement with ThermoFisher. We have certain payment obligations under the sub-license agreement including an upfront license fee of $665,000, which has already been paid, minimum annual royalty (in the tens of thousands of U.S. dollars prior to product approval and thereafter at a level of 50% of running royalties in the previous year), milestone payments (payable for each sub-licensed product on achievement of certain development and commercialization milestones per sub-licensed product) and a low single-digit running royalty payable on the net selling price of each sub-licensed product. The sub-license agreement will last until the expiration of the latest to expire of the sub-licensed patent rights. The sub-license agreement can be terminated before the end of its term by mutual agreement, by ThermoFisher or the head licensors on the occurrence of certain events (failure to use reasonable commercial efforts, willful making of a false statement of a material fact, failure to adequately meet any requirement for public use required under Federal regulations, breach of antitrust laws or other laws, material breach of the agreement, payment default or if we have challenged the validity or enforceability of any of the sub-licensed patents). The sub-license may also be terminated in the event of insolvency by either party. The sub-license has an additional requirement that any manufacture of engineered TCR products for sale in the United States must occur in the United States and reserves rights for the U.S. government to use the technology in accordance with 35 USC §200 et seq. and for the University of Michigan, and Dana-Farber Cancer Institute to use the technology for non-commercial research purposes. The aggregate milestone payments payable per product under the license and sub-license agreements do not exceed $5 million.
On June 16, 2016, the Company entered into a supply agreement with ThermoFisher for the supply of the Dynabeads® CD3/CD28 technology. The Dynabeads® CD3/CD28 technology is used in our manufacturing process to isolate, activate and expand patient T-cells. The supply agreement runs until December 31, 2025. Under the supply agreement, the Company
15
Table of Contents
is required to purchase its requirements for CD3/CD28 magnetic bead product exclusively from ThermoFisher for a period of 5 years and there are also minimum purchasing obligations. ThermoFisher has the right to terminate the supply agreement for material breach or insolvency.
See “Risk Factors—Risks Related to Our Reliance Upon Third Parties—We rely heavily on ThermoFisher and the technology we license from them.”
Immunocore Limited
We have an assignment and license agreement in place with Immunocore that relates to certain co-owned patents, patent applications and rights in know-how that originally was developed by Avidex and subsequently acquired by Medigene. Adaptimmune and Immunocore each utilize the jointly owned patents and know-how within separate fields or applications, with our focus being on the treatment of patients with our SPEAR T-cells and Immunocore’s focus being on the treatment of patients with soluble TCRs. There are no termination rights in the assignment and license agreement.
See further “Related “Risk Factors—Risks Related to Our Reliance Upon Third Parties—We have a shared development history with Immunocore and as a result jointly-own certainly intellectual property rights which are required for our ongoing business.”
Other Third-Party Intellectual Property Rights
Third-party patents do exist that purport to cover some or all of our current lentiviral vectors/systems or our process for manufacture. However, the majority of these patents will expire prior to any commercial supply by us of any TCR therapeutic candidates and we do not currently require a license. Whether licenses are required under any remaining third-party patents or other third-party patents depends on what steps we take going forward in relation to our lentiviral transduction process and manufacturing process. We may, however, need to negotiate a license under any remaining third party patents or develop alternative strategies for dealing with any remaining third party patents if licenses are not available on commercially acceptable terms or at all.
We are aware of a family of patent applications owned by The Board of Trustees of the University of Illinois which include two issued U.S. patents (U.S. 6,759,243 and 7,569,357) which were issued with very broad claims relating to high affinity TCRs. We believe that U.S. Patent 7,569,357, because of certain claim recitations, is not an impediment to the continued development of our current SPEAR T-cells. We requested re-examination of U.S. Patent 6,759,243 at the USPTO. In that re-examination, the USPTO adopted our position and rejected all claims under re-examination as anticipated or obvious, and in a related pending patent application of The Board of Trustees of the University of Illinois, in an August 18, 2014 Office Action, the USPTO also adopted our position and rejected the claims based on our arguments and evidence of our re-examination request. Through the re-examination process, we have been successful in achieving a narrowing of all of the claims of U.S. Patent 6,759,243. While we believe U.S. Patent 6,759,243 will be nonetheless invalid in the form in which it will be issued after re-examination, we do not believe the patent after re-examination will be an impediment to our current SPEAR T-cells, including inter alia because of the recitations added by the patentee during re-examination and the U.S. codified doctrine of “intervening rights.” Furthermore, these U.S. patents will likely expire prior to any commercial supply by us of any of our SPEAR T-cells. There are three European applications in this same family on which we have filed third party observations. Two of these applications have now been granted with claims narrowed away from Adaptimmune’s activities in such a way that we do not believe the patents should create an impediment to development of our current SPEAR T-cells within Europe. The third is still pending, but we expect the examiner again to accept the same arguments we used in the other two cases.
From time to time, we will use samples or cell lines obtained from third parties in order to identify either suitable targets or TCRs that bind to certain targets. The agreements under which samples are provided vary between third parties and certain third parties require entry into license agreements. These agreements may also contain payment obligations relating to the use of the various samples or the information obtained from use of those samples.
Laws and Regulations Regarding Patent Terms
The term of individual patents depends upon the legal term of the patents in the countries in which they are obtained. In most countries in which we file, the patent term is 20 years from the earliest date of filing a non-provisional patent application. In the United States, a patent term may be shortened if a patent is terminally disclaimed over another patent or as a result of delays in patent prosecution by the patentee. A patent’s term may be lengthened by a patent term adjustment, which compensates a patentee for administrative delays by the USPTO in granting a patent. The patent term of a European patent is 20 years from its effective filing date, which, unlike in the United States, is not subject to patent term adjustments in the same way as U.S. patents.
The term of a patent that covers an FDA-approved drug or biologic may also be eligible for patent term extension, which permits patent term restoration as compensation for the patent term lost during the FDA regulatory review process. The Drug Price Competition and Patent Term Restoration Act of 1984, or the Hatch-Waxman Act, permits a patent term extension of up to five years
16
Table of Contents
beyond the expiration of the patent. The length of the patent term extension is related to the length of time the drug or biologic is under regulatory review. Patent extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval and only one patent applicable to an approved drug may be extended. Similar provisions are available in Europe and other jurisdictions to extend the term of a patent that covers an approved drug, for example Supplementary Protection Certificates. In the future, if and when our products receive FDA approval or equivalent regulatory approval outside of the United States, we expect to apply for patent term extensions on patents covering those products. We anticipate that some of our issued patents may be eligible for patent term extensions, but such extensions may not be available and therefore our commercial monopoly may be restricted. See “Risk Factors—Risks Related to Our Intellectual Property—We may not be able to protect our proprietary technology in the marketplace or the cost of doing so may be prohibitive or excessive.”
Competition
The biotechnology and pharmaceutical industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. While we believe that our scientific knowledge, technology and development experience provide us with competitive advantages, we face potential competition from many different sources, including major pharmaceutical, specialty pharmaceutical and biotechnology companies, academic institutions, governmental agencies and public and private research institutions. Any TCR therapeutic candidates that we successfully develop and commercialize will compete with existing products and new products that may become available in the future.
Immunotherapy is an active area of research and a number of immune-related products have been identified in recent years that are alleged to modulate the immune system. Many of these products utilize dendritic cells, a form of immune cell that presents cancer target peptides to T cells and that can in turn result in T-cell activation.
More recently, bi-specific antibodies and checkpoint inhibitors have been identified as having utility in the treatment of cancer. Bi-specific antibodies commonly target both the cancer peptide and the TCR, thus bringing both cancer cells and T cells into close proximity to maximize the chance of TCR binding and hence an immune response to the cancer cells. Checkpoint inhibitors on the other hand work by targeting receptors that inhibit T-cell effectiveness and proliferation and essentially activate the T cells.
Other engineered T-cell therapeutics have also been identified using antibody recognition systems engineered into T cells, so-called CAR-T cells. These and other competitors in the TCR space include: Juno Therapeutics Inc., Kite Pharma Inc. / National Institutes of Health (“NIH”), Medigene AG/Bluebird Bio, Inc., Eureka Therapeutics Inc., Ziopharm Oncology, Inc. and Takara Bio Inc. In the CAR-T space, competitors include: Bellicum Pharmaceuticals, Inc., bluebird bio, Inc. / Celgene Corporation / Baylor College of Medicine, Cellectis SA / Pfizer Inc., Juno Therapeutics Inc. / Celgene Corporation / Fred Hutchinson Cancer Research Center / Memorial Sloan Kettering Cancer Center, Kite Pharma, Inc. / Amgen, Inc. / NIH/, Intrexon Corporation / Ziopharm Oncology, Inc. / MD Anderson Cancer Center and Novartis AG / University of Pennsylvania.
We do not believe that any of these competitors offer the same form of affinity-enhancement and specificity as our engineered TCR therapeutic candidates and, due to the low presentation of target peptide-HLA antigen on relevant cancer cells, those with TCR-based approaches are unlikely to be as effective. For example, Kite Pharma Inc. is in the process of, among other things, developing genetically engineered T-cells that bind directly to cancer cells. We believe this technology relies on the modification of T cells to express certain cancer-specific receptors, namely TCRs and CAR-Ts. Novartis also has substantial interest in the development of CAR-Ts. Juno Therapeutics Inc. has developed an engineered TCR therapeutic candidate where the end TCR is purported to have enhanced affinity through stem-cell selection. The therapeutic is produced in a very different way from the affinity-enhanced TCRs we produce, and we believe there is limited ability to control the enhancement obtained. Takara Bio Inc. has developed a naturally occurring TCR that binds to a MAGE A-4 target peptide and the therapeutic is in clinical trials. The TCR is not affinity-enhanced as is the TCR for our SPEAR T-cells. Medigene AG has also reported development of a PRAME TCR therapeutic candidate and is collaborating on a MAGE-A1 TCR which is due to enter clinical trials later in 2017. Eureka Therapeutics Inc. has announced the development of CAR-T products which target peptide-HLA complexes. They have developed CAR-Ts targeting the same NY-ESO and AFP peptides as are targeted by our SPEAR T-cells. However, development still appears to be in the early stages and limited data is available to assess impact on our own SPEAR T-cells, if any. Ziopharm Oncology, Inc. has announced the development of a TCR mimetic CAR-T targeting NY-ESO-1. Adicet Bio/Regeneron Inc. has announced plans to develop TCR immunotherapy products directed to MHC-peptide complexes and Tactiva Therapeutics are developing CD-4-TCRs and CD8-TCRs targeting solid tumors expressing NY-ESO. Guangzhou Xiangxue have published a number of patent applications for TCR immunotherapy products and we understand that the company are putting an NY-ESO-1 TCR into phase I clinical trials.
Immune Design Corp. has a vaccine in clinical trials which is not TCR-based. The vaccine targets the NY-ESO peptide in humans and again relies on binding to target peptides presented at low levels on target cells to stimulate natural low affinity T-cell responses. The treatment is not patient-specific.
17
Table of Contents
Government Regulation and Product Approvals
Government authorities in the United States, at the federal, state and local level, and in other countries and jurisdictions, including the European Union, extensively regulate, among other things, the research, development, testing, manufacture, quality control, approval, packaging, storage, recordkeeping, labeling, advertising, promotion, distribution, marketing, post-approval monitoring and reporting, and import and export of pharmaceutical products. The processes for obtaining regulatory approvals in the United States and in foreign countries and jurisdictions, along with subsequent compliance with applicable statutes and regulations and other regulatory authorities, require the expenditure of substantial time and financial resources.
The failure to comply with applicable U.S. requirements at any time during the product development process, approval process or after approval may subject an applicant and/or sponsor to a variety of administrative or judicial sanctions, including refusal by the FDA to approve pending applications, withdrawal of an approval, imposition of a clinical hold, issuance of warning letters and other types of letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement of profits, or civil or criminal investigations and penalties brought by the FDA and the Department of Justice (“DOJ”), or other governmental entities.
FDA Approval Process
In the United States, therapeutic products, including drugs, biologics, and medical devices are subject to extensive regulation by the FDA. The Federal Food, Drug, and Cosmetic Act (the “FDC Act”), and other federal and state statutes and regulations, govern, among other things, the research, development, testing, manufacture, storage, recordkeeping, approval, labeling, promotion and marketing, distribution, post-approval monitoring and reporting, sampling, and import and export of pharmaceutical products. Some biological products are subject to regulation under the FDC Act. Most biological products are approved for marketing under provisions of the Public Health Service Act (“PHSA”) via a Biologics License Application (“BLA”). The application process and requirements for approval of BLAs are generally similar to those for new drug applications (“NDAs”), and biologics are associated with generally similar, if not greater, approval risks and costs as drugs. Failure to comply with applicable U.S. requirements may subject a company to a variety of administrative or judicial sanctions, such as FDA refusal to approve pending NDAs or BLAs, warning or untitled letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, civil penalties, and criminal prosecution.
Biological product development for a new product or certain changes to an approved product in the United States typically involves preclinical laboratory and animal tests, the submission to the FDA of an IND, which must become effective before human clinical testing may commence, and adequate and well-controlled clinical trials to establish the safety and effectiveness of the drug for each indication for which FDA approval is sought. Satisfaction of FDA pre-market approval requirements typically takes many years and the actual time required may vary substantially based upon the type, complexity, and novelty of the product or disease.
Preclinical tests include laboratory evaluation of product chemistry, formulation, and toxicity, as well as animal trials to assess the characteristics and potential safety and efficacy of the product. The conduct of the preclinical tests must comply with federal regulations and requirements, including good laboratory practices. The results of preclinical testing are submitted to the FDA as part of an IND along with other information, including information about product chemistry, manufacturing and controls, and a proposed clinical trial protocol. Long term preclinical tests, such as animal tests of reproductive toxicity and carcinogenicity, may continue after the IND is submitted.
A 30-day waiting period after the submission of each IND is required prior to the commencement of clinical testing in humans. If the FDA has neither commented on nor questioned the IND within this 30-day period, the clinical trial proposed in the IND may begin.
Clinical trials involve the administration of the investigational biologic to healthy volunteers or patients under the supervision of a qualified investigator. Clinical trials must be conducted: (i) in compliance with federal regulations; (ii) in compliance with good clinical practice, or GCP, an international standard meant to protect the rights and health of patients and to define the roles of clinical trial sponsors, administrators, and monitors; as well as (iii) under protocols detailing the objectives of the trial, the parameters to be used in monitoring safety, and the effectiveness criteria to be evaluated. Each protocol involving testing on U.S. patients and subsequent protocol amendments must be submitted to the FDA as part of the IND.
The FDA may order the temporary, or permanent, discontinuation of a clinical trial at any time, or impose other sanctions, if it believes that the clinical trial either is not being conducted in accordance with FDA requirements or presents an unacceptable risk to the clinical trial patients. The trial protocol and informed consent information for patients in clinical trials must also be submitted to an IRB for approval. An IRB may also require the clinical trial at the site to be halted, either temporarily or permanently, for failure to comply with the IRB’s requirements, or may impose other conditions.
Clinical trials to support BLAs for marketing approval are typically conducted in three sequential phases, but the phases may overlap. In Phase 1, the initial introduction of the biologic into healthy human subjects or patients, the product is tested to assess metabolism, pharmacokinetics, pharmacological actions, side effects associated with increasing doses, and, if possible, early evidence
18
Table of Contents
on effectiveness. Phase 2 usually involves trials in a limited patient population to determine the effectiveness of the drug or biologic for a particular indication, dosage tolerance, and optimum dosage, and to identify common adverse effects and safety risks. If a compound demonstrates evidence of effectiveness and an acceptable safety profile in Phase 2 evaluations, Phase 3 trials are undertaken to obtain the additional information about clinical efficacy and safety in a larger number of patients, typically at geographically dispersed clinical trial sites, to permit the FDA to evaluate the overall benefit-risk relationship of the drug or biologic and to provide adequate information for the labeling of the product.
In most cases, the FDA requires two adequate and well-controlled Phase 3 clinical trials to demonstrate the efficacy of the biologic. A single Phase 3 trial with other confirmatory evidence may be sufficient in some instances where the trial is a large multicenter trial demonstrating internal consistency and a statistically very persuasive finding of a clinically meaningful effect on mortality, irreversible morbidity or prevention of a disease with a potentially serious outcome and confirmation of the result in a second trial would be practically or ethically impossible.
After completion of the required clinical testing, a BLA is prepared and submitted to the FDA. FDA approval of the BLA is required before marketing of the product may begin in the United States. The BLA must include the results of all preclinical, clinical, and other testing and a compilation of data relating to the product’s pharmacology, chemistry, manufacture, and controls. The cost of preparing and submitting a BLA is substantial. The submission of most BLAs is additionally subject to a substantial application user fee, currently exceeding $2,335,000, and the manufacturer and/or sponsor under an approved new drug application are also subject to annual product and establishment user fees, currently exceeding $110,000 per product and $569,000 per establishment. These fees are typically increased annually.
The FDA has 60 days from its receipt of a BLA to determine whether the application will be accepted for filing based on the agency’s threshold determination that it is sufficiently complete to permit substantive review. Once the submission is accepted for filing, the FDA begins an in-depth review. The FDA has agreed to certain performance goals in the review of BLAs. Most such applications for standard review biologic products are reviewed within 10 months of the date the FDA files the BLA; most applications for priority review biologics are reviewed within six months of the date the FDA files the BLA. Priority review can be applied to a biologic that the FDA determines has the potential to treat a serious or life-threatening condition and, if approved, would be a significant improvement in safety or effectiveness compared to available therapies. The review process for both standard and priority review may be extended by the FDA for three additional months to consider certain late-submitted information, or information intended to clarify information already provided in the submission.
The FDA may also refer applications for novel biologic products, or biologic products that present difficult questions of safety or efficacy, to an advisory committee—typically a panel that includes clinicians and other experts—for review, evaluation, and a recommendation as to whether the application should be approved. The FDA is not bound by the recommendation of an advisory committee, but it generally follows such recommendations. Before approving a BLA, the FDA will typically inspect one or more clinical sites to assure compliance with GCP. Additionally, the FDA will inspect the facility or the facilities at which the biologic product is manufactured. The FDA will not approve the product unless compliance with current good manufacturing practice cGMP is satisfactory and the BLA contains data that provide substantial evidence that the biologic is safe, pure, potent and effective in the indication studied.
After the FDA evaluates the BLA and the manufacturing facilities, it issues either an approval letter or a complete response letter. A complete response letter generally outlines the deficiencies in the submission and may require substantial additional testing, or information, in order for the FDA to reconsider the application. If, or when, those deficiencies have been addressed to the FDA’s satisfaction in a resubmission of the BLA, the FDA will issue an approval letter. The FDA has committed to reviewing such resubmissions in two or six months depending on the type of information included.
An approval letter authorizes commercial marketing of the biologic with specific prescribing information for specific indications. As a condition of BLA approval, the FDA may require a risk evaluation and mitigation strategy (“REMS”) to help ensure that the benefits of the biologic outweigh the potential risks. REMS can include medication guides, communication plans for healthcare professionals, and elements to assure safe use (“ETASU”). ETASU can include, but are not limited to, special training or certification for prescribing or dispensing, dispensing only under certain circumstances, special monitoring, and the use of patient registries. The requirement for a REMS can materially affect the potential market and profitability of the product. Moreover, product approval may require substantial post-approval testing and surveillance to monitor the product’s safety or efficacy. Once granted, product approvals may be withdrawn if compliance with regulatory standards is not maintained or problems are identified following initial marketing.
Changes to some of the conditions established in an approved application, including changes in indications, labeling, or manufacturing processes or facilities, may require submission and FDA approval of a new BLA or BLA supplement before the change can be implemented. A BLA supplement for a new indication may require clinical data similar to that in the original application, and the FDA uses the same procedures and actions in reviewing BLA supplements as it does in reviewing BLAs.
19
Table of Contents
FDA Guidance Governing Gene Therapy Products
The FDA has issued various guidance documents regarding gene therapies, which outline additional factors that the FDA will consider at each of the above stages of development and relate to, among other things, the proper preclinical assessment of gene therapies; the chemistry, manufacturing, and controls information that should be included in an IND application; the proper design of tests to measure product potency in support of an IND application or BLA; and measures to observe delayed adverse effects in subjects who have been exposed to investigational gene therapies when the risk of such effects is high.
If a gene therapy trial is conducted at, or sponsored by, institutions receiving NIH funding for recombinant DNA research, a protocol and related documentation must be submitted to, and the study registered with, the NIH Office of Biotechnology Activities (“OBA”), pursuant to the NIH Guidelines for Research Involving Recombinant DNA Molecules, prior to the submission of an IND to the FDA. In addition, many companies and other institutions not subject to the NIH Guidelines voluntarily follow them. The NIH convenes the RAC, a federal advisory committee, to discuss protocols that raise novel or particularly important scientific, safety or ethical considerations at one of its quarterly public meetings. The OBA notifies the FDA of the RAC’s decision regarding the necessity for full public review of a gene therapy protocol. RAC proceedings and reports are posted to the OBA website and may be accessed by the public.
Fast Track Designation and Accelerated Approval
The FDA is required to facilitate the development, and expedite the review, of biologics that are intended for the treatment of a serious or life- threatening disease or condition for which there is no effective treatment and which demonstrate the potential to address unmet medical needs for the condition. Under the fast track program, the sponsor of a new biologic candidate may request that the FDA designate the candidate for a specific indication as a fast track biologic concurrent with, or after, the filing of the IND for the candidate. The FDA must determine if the biologic candidate qualifies for fast track designation within 60 days of receipt of the sponsor’s request.
Under the fast track program and FDA’s accelerated approval regulations, the FDA may approve a biologic for a serious or life-threatening illness that provides meaningful therapeutic benefit to patients over existing treatments based upon a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments.
In clinical trials, a surrogate endpoint is a measurement of laboratory or clinical signs of a disease or condition that substitutes for a direct measurement of how a patient feels, functions, or survives. Surrogate endpoints can often be measured more easily or more rapidly than clinical endpoints. A biologic candidate approved on this basis is subject to rigorous post- marketing compliance requirements, including the completion of Phase 4 or post-approval clinical trials to confirm the effect on the clinical endpoint. Failure to conduct required post-approval trials, or confirm a clinical benefit during post-marketing trials, will allow the FDA to withdraw the biologic from the market on an expedited basis. All promotional materials for biologic candidates approved under accelerated regulations are subject to prior review by the FDA.
In addition to other benefits such as the ability to use surrogate endpoints and engage in more frequent interactions with the FDA, the FDA may initiate review of sections of a fast track product’s BLA before the application is complete. This rolling review is available if the applicant provides, and the FDA approves, a schedule for the submission of the remaining information and the applicant pays applicable user fees. However, the FDA’s time period goal for reviewing an application does not begin until the last section of the BLA is submitted. Additionally, the fast track designation may be withdrawn by the FDA if the FDA believes that the designation is no longer supported by data emerging in the clinical trial process.
Breakthrough Therapy Designation
The FDA is also required to expedite the development and review of the application for approval of biological products that are intended to treat a serious or life-threatening disease or condition where preliminary clinical evidence indicates that the biologic may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints.
Under the breakthrough therapy program, the sponsor of a new biologic candidate may request that the FDA designate the candidate for a specific indication as a breakthrough therapy concurrent with, or after, the filing of the IND for the biologic candidate. The FDA must determine if the biological product qualifies for breakthrough therapy designation within 60 days of receipt of the sponsor’s request.
Orphan Drug Designation
Under the Orphan Drug Act, the FDA may grant orphan drug designation to biological products intended to treat a rare disease or condition, generally a disease or condition that affects fewer than 200,000 individuals in the United States, or if it affects more than 200,000 individuals in the United States, there is no reasonable expectation that the cost of developing and making a
20
Table of Contents
product available in the United States for such disease or condition will be recovered from sales of the product. Orphan drug designation must be requested before submitting a BLA. After the FDA grants orphan drug designation, the identity of the biological product and its potential orphan use are disclosed publicly by the FDA. Orphan drug designation does not convey any advantage in, or shorten the duration of, the regulatory review and approval process. The first BLA applicant to receive FDA approval for a particular active moiety to treat a particular disease with FDA orphan drug designation is entitled to a seven-year exclusive marketing period in the United States for that product for that indication. During the seven-year exclusivity period, the FDA may not approve any other applications to market a biological product containing the same active moiety for the same disease, except in limited circumstances, such as a showing of clinical superiority to the product with orphan drug exclusivity. A product is clinically superior if it is safer, more effective or makes a major contribution to patient care. Orphan drug exclusivity does not prevent the FDA from approving a different drug or biological product for the same disease or condition, or the same biological product for a different disease or condition. Among the other benefits of orphan drug designation are tax credits for certain research and a waiver of the BLA user fee.
Disclosure of Clinical Trial Information
Sponsors of human clinical trials of FDA-regulated products, including biological products, are required to register and disclose certain clinical trial information. Information related to the product, patient population, phase of investigation, trial sites and investigators, and other aspects of the clinical trial is then made public as part of the registration. Sponsors are also obligated to discuss the results of their clinical trials after completion. Disclosure of the results of these trials can be delayed until the new product or new indication being studied has been approved. Competitors may use this publicly available information to gain knowledge regarding the progress of development programs.
Pediatric Information
Under the Pediatric Research Equity Act, or PREA, NDAs or BLAs or supplements to NDAs or BLAs must contain data to assess the safety and effectiveness of the biological product for the claimed indications in all relevant pediatric subpopulations and to support dosing and administration for each pediatric subpopulation for which the biological product is safe and effective. The FDA may grant full or partial waivers, or deferrals, for submission of data. Unless otherwise required by regulation, PREA does not apply to any biological product for an indication for which orphan designation has been granted.
Additional Controls for Biologics
To help reduce the increased risk of the introduction of adventitious agents, the PHSA emphasizes the importance of manufacturing controls for products whose attributes cannot be precisely defined. The PHSA also provides authority to the FDA to immediately suspend licenses in situations where there exists a danger to public health, to prepare or procure products in the event of shortages and critical public health needs, and to authorize the creation and enforcement of regulations to prevent the introduction or spread of communicable diseases in the United States and between states.
After a BLA is approved, the product may also be subject to official lot release as a condition of approval. As part of the manufacturing process, the manufacturer is required to perform certain tests on each lot of the product before it is released for distribution. If the product is subject to official release by the FDA, the manufacturer submits samples of each lot of product to the FDA together with a release protocol showing a summary of the history of manufacture of the lot and the results of all of the manufacturer’s tests performed on the lot. The FDA may also perform certain confirmatory tests on lots of some products, such as viral vaccines, before releasing the lots for distribution by the manufacturer. In addition, the FDA conducts laboratory research related to the regulatory standards on the safety, purity, potency, and effectiveness of biological products. As with drugs, after approval of biologics, manufacturers must address any safety issues that arise, are subject to recalls or a halt in manufacturing, and are subject to periodic inspection after approval.
Biosimilars
The Biologics Price Competition and Innovation Act of 2009, or BPCIA, created an abbreviated approval pathway for biological products shown to be highly similar to or interchangeable with an FDA-licensed reference biological product. Under the BPCIA, a biological product may be deemed biosimilar to an FDA-approved biological product or reference biological product upon a showing that there are no differences in conditions of use, route of administration, dosage form, and strength, and no clinically meaningful differences between the biological product and the reference product in terms of safety, purity, and potency. Biosimilarity generally must be shown through analytical trials, animal trials, and a clinical trial or trials, unless the Secretary waives a required element. A biosimilar product may be deemed interchangeable with a prior approved product if it meets the higher hurdle of demonstrating that it can be expected to produce the same clinical results as the reference product and, for products administered multiple times, the biologic and the reference biologic may be switched after one has been previously administered without increasing safety risks or risks of diminished efficacy relative to exclusive use of the reference biologic. On March 6, 2015, the FDA approved the first biosimilar product under the BPCIA. Complexities associated with the larger, and often more complex, structures of biological products, as well as the process by which such products are manufactured, pose significant hurdles to implementation, which is still being evaluated by the FDA.
21
Table of Contents
A reference biologic is granted 12 years of marketing exclusivity from the time of first licensure of the reference product, and in addition no application for a biosimilar can be submitted for four years from the date of licensure of the reference product. The first biologic product submitted under the abbreviated approval pathway that is determined to be interchangeable with the reference product has exclusivity against a finding of interchangeability for other biologics for the same condition of use for the lesser of (i) one year after first commercial marketing of the first interchangeable biosimilar, (ii) eighteen months after the first interchangeable biosimilar is approved if there is no patent challenge, (iii) eighteen months after resolution of a lawsuit over the patents of the reference biologic in favor of the first interchangeable biosimilar applicant, or (iv) 42 months after the first interchangeable biosimilar’s application has been approved if a patent lawsuit is ongoing within the 42-month period.
Post-Approval Requirements
Once a BLA is approved, a product will be subject to certain post-approval requirements. For instance, the FDA closely regulates the post-approval marketing and promotion of biologics, including standards and regulations for direct-to-consumer advertising, off-label promotion, industry- sponsored scientific and educational activities and promotional activities involving the internet. Biologics may be marketed only for the approved indications and in accordance with the provisions of the approved labeling.
Adverse event reporting and submission of periodic reports is required following FDA approval of a BLA. The FDA also may require post-marketing testing, known as Phase 4 testing, REMS, and surveillance to monitor the effects of an approved product, or the FDA may place conditions on an approval that could restrict the distribution or use of the product. In addition, quality control, biological product manufacture, packaging, and labeling procedures must continue to conform to cGMPs after approval. Biologic manufacturers and certain of their subcontractors are required to register their establishments with the FDA and certain state agencies. Registration with the FDA subjects entities to periodic unannounced inspections by the FDA, during which the agency inspects manufacturing facilities to assess compliance with cGMPs. Accordingly, manufacturers must continue to expend time, money, and effort in the areas of production and quality-control to maintain compliance with cGMPs. Regulatory authorities may withdraw product approvals or request product recalls if a company fails to comply with regulatory standards, if it encounters problems following initial marketing, or if previously unrecognized problems are subsequently discovered.
FDA Regulation of Companion Diagnostics
If safe and effective use of a therapeutic product depends on an in vitro diagnostic, then the FDA generally will require approval or clearance of the diagnostic, known as a companion diagnostic, at the same time that the FDA approves the therapeutic product. The FDA has generally required in vitro companion diagnostics intended to select the patients who will respond to cancer treatment to obtain marketing approval through the pre-market approval (“PMA”) process for that diagnostic simultaneously with approval of the therapeutic. The review of these in vitro companion diagnostics in conjunction with the review of a cancer therapeutic involves coordination of review by the FDA’s Center for Biologics Evaluation and Research and by the FDA’s Center for Devices and Radiological Health.
The PMA process, including the gathering of clinical and preclinical data and the submission to and review by the FDA, can take several years or longer. It involves a rigorous premarket review during which the applicant must prepare and provide the FDA with reasonable assurance of the device’s safety and effectiveness and information about the device and its components regarding, among other things, device design, manufacturing and labeling. PMA applications are subject to an application fee, which exceeds $250,000 for most PMAs. In addition, PMAs for certain devices must generally include the results from extensive preclinical and adequate and well-controlled clinical trials to establish the safety and effectiveness of the device for each indication for which FDA approval is sought. In particular, for a diagnostic, the applicant must demonstrate that the diagnostic produces reproducible results when the same sample is tested multiple times by multiple users at multiple laboratories. As part of the PMA review, the FDA will typically inspect the manufacturer’s facilities for compliance with the Quality System Regulation, or QSR, which imposes elaborate testing, control, documentation and other quality assurance requirements.
PMA approval is not guaranteed, and the FDA may ultimately respond to a PMA submission with a not approvable determination based on deficiencies in the application and require additional clinical trial or other data that may be expensive and time-consuming to generate and that can substantially delay approval. If the FDA finds the PMA application is approvable, the FDA typically issues an approvable letter requiring the applicant’s agreement to specific conditions, such as changes in labeling, or specific additional information, such as submission of final labeling, in order to secure final approval of the PMA. If the FDA concludes that the applicable criteria have been met, the FDA will issue a PMA for the approved indications, which can be more limited than those originally sought by the applicant. The PMA can include post-approval conditions that the FDA believes necessary to ensure the safety and effectiveness of the device, including, among other things, restrictions on labeling, promotion, sale and distribution.
22
Table of Contents
After a device is placed on the market, it remains subject to significant regulatory requirements. Medical devices may be marketed only for the uses and indications for which they are cleared or approved. Device manufacturers must also establish registration and device listings with the FDA. A medical device manufacturer’s manufacturing processes and those of its suppliers are required to comply with the applicable portions of the QSR, which cover the methods and documentation of the design, testing, production, processes, controls, quality assurance, labeling, packaging and shipping of medical devices. Domestic facility records and manufacturing processes are subject to periodic unscheduled inspections by the FDA. The FDA also may inspect foreign facilities that export products to the United States.
Anti-Kickback, False Claims Laws
In addition to FDA restrictions on marketing of pharmaceutical products, several other types of state and federal laws have been applied to restrict certain marketing practices in the pharmaceutical industry in recent years. These laws include anti-kickback statutes, false claims statutes, and other statutes pertaining to health care fraud and abuse. The federal healthcare program anti-kickback statute prohibits, among other things, knowingly and willfully offering, paying, soliciting or receiving remuneration to induce, or in return for, purchasing, leasing, ordering or arranging for the purchase, lease or order of any healthcare item or service reimbursable under Medicare, Medicaid, or other federally financed healthcare programs. The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, collectively, the Healthcare Reform Act, amended the intent element of the federal statute so that a person or entity no longer needs to have actual knowledge of the statute or specific intent to violate it. This statute has been interpreted to apply to arrangements between pharmaceutical manufacturers on the one hand and prescribers, purchasers, and formulary managers on the other. Violations of the anti-kickback statute are punishable by imprisonment, criminal fines, civil monetary penalties, and exclusion from participation in federal healthcare programs. Although there are a number of statutory exemptions and regulatory safe harbors protecting certain common activities from prosecution or other regulatory sanctions, the exemptions and safe harbors are drawn narrowly, and practices that involve remuneration intended to induce prescribing, purchases, or recommendations may be subject to scrutiny if they do not qualify for an exemption or safe harbor.
Federal false claims laws prohibit any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government, or knowingly making, or causing to be made, a false statement to have a false claim paid. This includes claims made to programs where the federal government reimburses, such as Medicaid, as well as programs where the federal government is a direct purchaser, such as when it purchases off the Federal Supply Schedule. Recently, several pharmaceutical and other healthcare companies have been prosecuted under these laws for allegedly inflating drug prices they report to pricing services, which in turn were used by the government to set Medicare and Medicaid reimbursement rates, and for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product.
In addition, certain marketing practices, including off-label promotion, may also violate false claims laws. Additionally, the Healthcare Reform Act amended the federal false claims law such that a violation of the federal healthcare program anti-kickback statute can serve as a basis for liability under the federal false claims law. The majority of states also have statutes or regulations similar to the federal anti-kickback law and false claims laws, which apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payor.
Other federal statutes pertaining to healthcare fraud and abuse include the civil monetary penalties statute, which prohibits the offer or payment of remuneration to a Medicaid or Medicare beneficiary that the offerer/payor knows or should know is likely to influence the beneficiary to order a receive a reimbursable item or service from a particular supplier, and the healthcare fraud statute, which prohibits knowingly and willfully executing or attempting to execute a scheme to defraud any healthcare benefit program or obtain by means of false or fraudulent pretenses, representations, or promises any money or property owned by or under the control of any healthcare benefit program in connection with the delivery of or payment for healthcare benefits, items, or services.
Other Federal and State Regulatory Requirements
The Centers for Medicare & Medicaid Services, or CMS, has issued a final rule that implements a statutory requirement under the Healthcare Reform Act that requires applicable manufacturers of drugs, devices, biologicals, or medical supplies that are covered under Medicare, Medicaid, or the Children’s Health Insurance Program, or CHIP, to begin collecting and reporting annually information on payments or transfers of value to physicians and teaching hospitals, as well as investment interests held by physicians and their immediate family members. Manufacturers had to begin collecting information in 2013, with the first reports due in 2014. On September 30, 2014, CMS posted the first round of data in searchable form on a public website. Failure to submit required information may result in civil monetary penalties.
In addition, several states now require prescription drug companies to report expenses relating to the marketing and promotion of drug products and to report gifts and payments to individual physicians in these states. Other states prohibit various other marketing-related activities. Still other states require the posting of information relating to clinical trials and their outcomes. In addition, California, Connecticut, Nevada, and Massachusetts require pharmaceutical companies to implement compliance programs and/or marketing codes. Several additional states are considering similar proposals. Compliance with these laws is difficult and time consuming, and companies that do not comply with these state laws face civil penalties.
23
Table of Contents
Europe and Rest of the World Regulation
In addition to regulations in the United States, we will be subject to a variety of regulations in other jurisdictions both due to our location and the fact that we are engaging in clinical programs outside of the United States and will want to obtain worldwide regulatory approval for our TCR therapeutic candidates. Prior to supplying any TCR therapeutic candidate in any country or starting any clinical trials in any country outside of the United States we must obtain the requisite approvals from regulatory authorities in such countries. The existence of a United States regulatory approval does not guarantee that regulatory approvals will be obtained in other countries in which we wish to conduct clinical trials or market our TCR therapeutic candidates. In the EU, for example, a clinical trial application must be submitted to each country’s national health authority and an independent ethics committee, much like the FDA and IRB, respectively prior to any clinical trial being conducted in the relevant country. A marketing authorization is then submitted prior to any commercial supply, again to each relevant country’s national health authority.
The requirements and process governing the conduct of clinical trials, product licensing, pricing and reimbursement vary from country to country. In all cases, the clinical trials are conducted in accordance with GCP and the applicable regulatory requirements and the ethical principles that have their origin in the Declaration of Helsinki. However these requirements may well differ from country to country.
Review and Approval of Drug Products outside of the United States
In order to market any product outside of the United States, a company must also comply with numerous and varying regulatory requirements of other countries and jurisdictions regarding quality, safety and efficacy and governing, among other things, clinical trials, marketing authorization, commercial sales and distribution of products. Whether or not it obtains FDA approval for a product, the company would need to obtain the necessary approvals by the comparable foreign regulatory authorities before it can commence clinical trials or marketing of the product in those countries or jurisdictions. The approval process ultimately varies between countries and jurisdictions and can involve additional product testing and additional administrative review periods. The time required to obtain approval in other countries and jurisdictions might differ from and be longer than that required to obtain FDA approval. Regulatory approval in one country or jurisdiction does not ensure regulatory approval in another, but a failure or delay in obtaining regulatory approval in one country or jurisdiction may negatively impact the regulatory process in others.
Procedures Governing Approval of Products in the EU
Pursuant to the European Clinical Trials Directive, a system for the approval of clinical trials in the European Union has been implemented through national legislation of the member states. Under this system, an applicant must obtain approval from the competent national authority of a European Union member state in which the clinical trial is to be conducted. Furthermore, the applicant may only start a clinical trial after a competent ethics committee has issued a favorable opinion. Clinical trial application must be accompanied by an investigational medicinal product dossier with supporting information prescribed by the European Clinical Trials Directive and corresponding national laws of the member states and further detailed in applicable guidance documents.
To obtain marketing approval of a product under European Union regulatory systems, an applicant must submit a marketing authorization application, or MAA, either under a centralized or decentralized procedure. The centralized procedure provides for the grant of a single marketing authorization by the European Commission that is valid for all European Union member states. The centralized procedure is compulsory for specific products, including for medicines produced by certain biotechnological processes, products designated as orphan medicinal products, advanced therapy products and products with a new active substance indicated for the treatment of certain diseases. For products with a new active substance indicated for the treatment of other diseases and products that are highly innovative or for which a centralized process is in the interest of patients, the centralized procedure may be optional.
Under the centralized procedure, the Committee for Medicinal Products for Human Use, or the CHMP, established at the EMA is responsible for conducting the initial assessment of a product. The CHMP is also responsible for several post-authorization and maintenance activities, such as the assessment of modifications or extensions to an existing marketing authorization. Under the centralized procedure in the European Union, the maximum timeframe for the evaluation of an MAA is 210 days, excluding clock stops, when additional information or written or oral explanation is to be provided by the applicant in response to questions of the CHMP. Accelerated evaluation might be granted by the CHMP in exceptional cases, when a medicinal product is of major interest from the point of view of public health and in particular from the viewpoint of therapeutic innovation. In this circumstance, the EMA ensures that the opinion of the CHMP is given within 150 days.
24
Table of Contents
The decentralized procedure is available to applicants who wish to market a product in various European Union member states where such product has not received marketing approval in any European Union member states before. The decentralized procedure provides for approval by one or more other, or concerned, member states of an assessment of an application performed by one member state designated by the applicant, known as the reference member state. Under this procedure, an applicant submits an application based on identical dossiers and related materials, including a draft summary of product characteristics, and draft labeling and package leaflet, to the reference member state and concerned member states. The reference member state prepares a draft assessment report and drafts of the related materials within 210 days after receipt of a valid application. Within 90 days of receiving the reference member state’s assessment report and related materials, each concerned member state must decide whether to approve the assessment report and related materials.
If a member state cannot approve the assessment report and related materials on the grounds of potential serious risk to public health, the disputed points are subject to a dispute resolution mechanism and may eventually be referred to the European Commission, whose decision is binding on all member states.
In order to market any product outside of the United States, a company must also comply with numerous and varying regulatory requirements of other countries and jurisdictions regarding quality, safety and efficacy and governing, among other things, clinical trials, marketing authorization, commercial sales and distribution of drug products. Whether or not it obtains FDA approval for a product, the company would need to obtain the necessary approvals by the comparable foreign regulatory authorities before it can commence clinical trials or marketing of the product in those countries or jurisdictions. The approval process ultimately varies between countries and jurisdictions and can involve additional product testing and additional administrative review periods. The time required to obtain approval in other countries and jurisdictions might differ from and be longer than that required to obtain FDA approval. Regulatory approval in one country or jurisdiction does not ensure regulatory approval in another, but a failure or delay in obtaining regulatory approval in one country or jurisdiction may negatively impact the regulatory process in others.
Marketing authorization is valid for five years in principle and the marketing authorization may be renewed after five years on the basis of a re-evaluation of the risk-benefit balance by the EMA or by the competent authority of the authorizing member state. To this end, the marketing authorization holder must provide the EMA or the competent authority with a consolidated version of the file in respect of quality, safety and efficacy, including all variations introduced since the marketing authorization was granted, at least six months before the marketing authorization ceases to be valid. Once renewed, the marketing authorization is valid for an unlimited period, unless the Commission or the competent authority decides, on justified grounds relating to pharmacovigilance, to proceed with one additional five-year renewal. Any authorization which is not followed by the actual placing of the drug on the EU market (in case of centralized procedure) or on the market of the authorizing member state within three years after authorization ceases to be valid (the so-called sunset clause).
Legal Proceedings and Related Matters
From time to time, we may be party to litigation that arises in the ordinary course of our business. We do not have any pending litigation that, separately or in the aggregate, would, in the opinion of management, have a material adverse effect on our results of operations, financial condition or cash flows.
Employees
As of December 31, 2016, we had 298 full-time equivalent employees. Of these employees, 232 were in research and development (including in manufacturing and operations, and quality control and quality assurance) and 66 were in management and administrative functions (including business development, finance, intellectual property, information technology and general administration). We have never had a work stoppage and none of our employees are covered by collective bargaining agreements or represented by a labor union. We believe our employee relations are good.
Available Information
Access to our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and amendments to these reports filed with or furnished to the SEC, may be obtained through the investor section of our website at www.adaptimmune.com as soon as reasonably practical after we electronically file or furnish these reports. We do not charge for access to and viewing of these reports. Information in the investor section and on our website is not part of this Annual Report on Form 10-K or any of our other securities filings unless specifically incorporated herein by reference. In addition, the public may read and copy any materials that we file with the SEC at the SEC’s Public Reference Room at 100 F Street, NE, Washington, D.C. 20549. The public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. Also, our filings with the SEC may be accessed through the SEC’s website at www.sec.gov. All statements made in any of our securities filings, including all forward-looking statements or information, are made as of the date of the document in which the statement is included, and we do not assume or undertake any obligation to update any of those statements or documents unless we are required to do so by law.
25
Table of Contents
Corporate Information
Adaptimmune Therapeutics plc was incorporated on December 3, 2014 and is a public limited company incorporated under the laws of England and Wales. Pursuant to a corporate reorganization, completed on April 1, 2015, Adaptimmune Therapeutics plc holds the entire issued share capital of Adaptimmune Limited. Prior to the corporate reorganization, our business was conducted by Adaptimmune Limited and its consolidated subsidiary. Adaptimmune Limited was incorporated on December 19, 2007. Subsequent to the corporate reorganization our business was conducted by Adaptimmune Therapeutics plc and its consolidated subsidiaries, including Adaptimmune Limited. Our registered and principal executive offices are located at 101 Park Drive, Milton Park, Abingdon, Oxfordshire OX14 4RY, United Kingdom, our general telephone number is (+44) 1235 430000 and our corporate website address is www.adaptimmune.com. Our website and the information contained on or accessible through our website are not part of this document. Our agent for service of process in the United States is Adaptimmune LLC, located at 351 Rouse Boulevard, The Navy Yard, Philadelphia PA 19112, United States.
26
Table of Contents
Item 1A. Risk Factors
Our business has significant risks. You should carefully consider the following risk factors as well as all other information contained in this Annual Report, including our condensed consolidated financial statements and the related notes, before making an investment decision regarding our securities. The risks and uncertainties described below are those significant risk factors currently known and specific to us that we believe are relevant to our business, results of operations and financial condition. Additional risks and uncertainties not currently known to us or that we now deem immaterial may also impair our business, results of operations and financial condition.
Risks Related to Our Financial Condition and Capital Requirements
We are a clinical-stage biopharmaceutical company with no commercial products and prediction of future performance is very difficult.
We are a clinical-stage biopharmaceutical company focused on novel cancer immunotherapy products. We have no products or therapeutics approved for commercial sale and have not generated any revenue from product supplies or royalties. Our therapeutic candidates are based on engineered TCRs and are new and largely unproven. Our limited operating history, particularly in light of the rapidly evolving cancer immunotherapy field, may make it difficult to evaluate our current business and predict our future performance. Investment in biopharmaceutical product development is highly speculative because it entails substantial upfront capital expenditures and significant risk that any potential product candidate will fail to demonstrate adequate effect or an acceptable safety profile, gain regulatory approval and become commercially viable. Our inability to address these risks successfully would have a materially adverse effect on our business and prospects.
We have incurred net losses every year since our inception and expect to continue to incur net losses in the future.
We have generated losses since our inception in 2008, during which time we have devoted substantially all of our resources to research and development efforts relating to our SPEAR T-cells, including engaging in activities to manufacture and supply our SPEAR T-cells for clinical trials in compliance with cGMP, conducting clinical trials of our SPEAR T-cells, providing general and administrative support for these operations and protecting our intellectual property. We do not have any products approved for sale and have not generated any revenue from product supplies or royalties. Based on our current plans, we do not expect to generate product or royalty revenues unless and until we obtain marketing approval for, and commercialize, any of our SPEAR T-cells.
For the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, we incurred net losses of $71.6 million, $23.0 million, $22.1 million, and $11.6 million, respectively. As of December 31, 2016, we had accumulated losses of $161.5 million. We expect to continue incurring significant losses as we continue with our research and development programs and to incur general and administrative costs associated with our operations. The extent of funding required to develop our product candidates is difficult to estimate given the novel nature of our SPEAR T-cells and their un-proven route to market. Our profitability is dependent upon the successful development, approval, and commercialization of our SPEAR T-cells, successfully achieving GSK milestones and achieving a level of revenues adequate to support our cost structure. We may never achieve profitability, and unless and until we do, we will continue to need to raise additional cash.
We have never generated any revenue from sales of our SPEAR T-cells and our ability to generate revenue from sales of our SPEAR T-cells and become profitable depends significantly on our success in a number of factors.
We have no SPEAR T-cells approved for commercial sale, have not generated any revenue from sales of our SPEAR T-cells, and do not anticipate generating any revenue from sales of our SPEAR T-cells until some time after we receive regulatory approval, if at all, for the commercial sale of a SPEAR T-cell. We intend to fund future operations through milestone payments under our collaboration and license agreement with GSK and through additional equity financings or other third party collaborations. Our ability to generate revenue and achieve profitability depends on our success in many factors, including:
· completing preclinical development and advancing our SPEAR T-cells to clinic;
· delivering on the clinical development strategy for our SPEAR T-cells;
· progressing our clinical trials within predicted timeframes and without any substantial delays, for example as may be caused by delays in patient recruitment, regulatory requirements to hold or suspend any clinical trials or delays in obtaining approvals required to conduct clinical trials;
27
Table of Contents
· demonstrating a favorable benefit (efficacy parameters): risk (safety) for our SPEAR T-cells that translate into a differentiated product of value for patients;
· obtaining data from clinical trials which are ongoing for SPEAR T-cells other than our NY-ESO SPEAR T-cell;
· obtaining regulatory approvals and marketing authorizations for our SPEAR T-cells for which we complete clinical trials;
· progressing our clinical trials within predicted timeframes and without any substantial delays, for example as may be caused by delays in patient recruitment, regulatory requirements to hold or suspend any clinical trials or delays in obtaining approvals required to conduct clinical trials;
· developing sustainable and scalable manufacturing and supply processes for our SPEAR T-cells, including establishing and maintaining commercially viable supply relationships with third parties and establishing our own commercial manufacturing capabilities and infrastructure;
· launching and commercializing SPEAR T-cells for which we obtain regulatory approvals and marketing authorizations, either directly or with a collaborator or distributor;
· obtaining market acceptance, pricing and reimbursement of our SPEAR T-cells as viable treatment options;
· addressing any competing technological and market developments;
· identifying, assessing, acquiring and/or developing new SPEAR T-cells;
· maintaining, protecting, and expanding our portfolio of intellectual property rights, including patents, trade secrets and know-how; and
· attracting, hiring and retaining qualified personnel.
Even if one or more of our SPEAR T-cells is approved for commercial sale, we anticipate incurring significant costs associated with commercializing any approved SPEAR T-cell. Our expenses could increase beyond expectations if the FDA or any other regulatory agency requires changes to our manufacturing processes or assays, or for us to perform preclinical programs and clinical or other types of trials in addition to those that we currently anticipate. If we are successful in obtaining regulatory approvals to market one or more of our SPEAR T-cells, our revenue will be dependent, in part, upon the size of the markets in the territories for which we gain regulatory approval, the accepted price for the SPEAR T-cell, the ability to get reimbursement at any price, and whether we own the commercial rights for that territory. If the number of our addressable disease patients is not as significant as we estimate, the indication approved by regulatory authorities is narrower than we expect, or the reasonably accepted population for treatment is narrowed by competition, physician choice or treatment guidelines, we may not generate significant revenue from sales or supplies of such SPEAR T-cells, even if approved. If we are not able to generate revenue from the sale of any approved SPEAR T-cells, we may never become profitable.
If we fail to obtain additional financing, we may be unable to complete the development and commercialization of our SPEAR T-cells.
Our operations have required substantial amounts of cash since inception. We expect to continue to spend substantial amounts to continue the development of our SPEAR T-cells, including future clinical trials. If we receive approval for any of our SPEAR T-cells, we will require significant additional amounts in order to launch and commercialize these therapeutic candidates.
As of December 31, 2016, we had $158.8 million of cash and cash equivalents and $22.7 million of short-term deposits. We expect to use these funds to advance and accelerate the clinical development of our MAGE-A10, MAGE-A4 and AFP SPEAR T-cells, to further develop and enhance our manufacturing capabilities and secure a commercially viable manufacturing platform for all of our SPEAR T-cells, to advance additional SPEAR T-cells into preclinical testing and progress such SPEAR T-cells through to clinical trials as quickly as possible and to fund working capital, including other general corporate purposes. We believe that such proceeds, our existing cash, and cash equivalents and short-term deposits together with milestones payments to us under the GSK Collaboration and License Agreement will be sufficient to fund our operations for the foreseeable future, including for at least the next 12 months. However, changing circumstances beyond our control, including changes to the scope and timing of the programs under the GSK collaboration, may cause us to increase our spending significantly faster than we currently anticipate. We may require additional capital for the further development and commercialization of our SPEAR T-cells and may need to raise additional funds sooner if we choose to expand more rapidly than we presently anticipate.
28
Table of Contents
We cannot be certain that additional funding will be available on acceptable terms, or at all. We have no committed source of additional capital and if we are unable to raise additional capital in sufficient amounts or on terms acceptable to us, we may have to significantly delay, scale back or discontinue the development or commercialization of our SPEAR T-cells or other research and development initiatives. Our license and supply agreements may also be terminated if we are unable to meet the payment obligations under these agreements. We could be required to seek collaborators for our SPEAR T-cells at an earlier stage than otherwise would be desirable or on terms that are less favorable than might otherwise be available or relinquish or license on unfavorable terms our rights to our SPEAR T-cells in markets where we otherwise would seek to pursue development or commercialization ourselves. Any of the above events could significantly harm our business, prospects, financial condition and results of operations and cause the price of our American Depositary Shares, or ADSs, to decline.
Risks Related to the Development of Our SPEAR T-cells
Our business is highly dependent on our lead NY-ESO SPEAR T-cell, which will require significant additional clinical testing before we can seek regulatory approval and begin commercialization of any of our SPEAR T-cells.
There is no guarantee that any of our SPEAR T-cells will achieve regulatory approval or proceed to the next stage of clinical programs. The process for obtaining marketing approval for any candidate is very long and risky and there will be significant challenges for us to address in order to obtain marketing approval, if at all.
There is no guarantee that the results obtained in current clinical trials for our NY-ESO SPEAR T-cell will be sufficient to plan one or more pivotal clinical trials and obtain regulatory approval or marketing authorization. Negative results in this lead clinical program of our NY-ESO SPEAR T-cell or in other investigator-initiated clinical programs utilizing our NY-ESO therapeutic candidate may also impact our ability to obtain regulatory approval for other SPEAR T-cells, either at all or within anticipated timeframes because, although the SPEAR T-cell may target a different cancer peptide, the underlying technology platform, manufacturing process and development process is the same for all of our SPEAR T-cells. Accordingly, a failure in any one program may affect the ability to obtain regulatory approval to continue or conduct clinical programs for other SPEAR T-cells.
We may not be able to submit INDs, or the foreign equivalent outside of the United States, to commence additional clinical trials for other SPEAR T-cells on the timeframes we expect, and even if we are able to, the FDA or comparable foreign regulatory authorities may not permit us to proceed with planned clinical trials.
Progression of new SPEAR T-cells into clinical trials is inherently risky and dependent on the results obtained in preclinical programs, the results of other clinical programs and results of third-party programs that utilize common components, such as production of the lentiviral vector lot used for production and administration of our SPEAR T-cell. If results are not available when expected or problems are identified during SPEAR T-cell development, we may experience significant delays in development of pipeline products and in existing clinical programs, which may impact our ability to receive regulatory approval. This may also impact our ability to achieve certain financial milestones and the expected timeframes to market any of our SPEAR T-cells. Failure to submit further IND or the foreign equivalent and commence additional clinical programs will significantly limit our opportunity to generate revenue.
There is no guarantee that the FDA, or any other regulatory authority, will approve any IND (or equivalent application) for any of our SPEAR T-cells, or for new indications for our SPEAR T-cells already in clinical trials, or that amendments to existing protocols will not be required. For example, the FDA issued a partial clinical hold for the Company’s proposed MRCLS trial with NY-ESO following review of the IND submitted for the trial. The FDA notification was not based on safety concerns. In its correspondence the FDA requested additional Chemistry Manufacturing and Controls, or CMC, and clinical information prior to the commencement of the proposed trial. An amendment to the ADP-0011-007 protocol for the trial was filed with the FDA which converted the trial into a pilot trial (rather than the previously proposed pivotal trial design with a futility phase) and this amended protocol has now been approved by the FDA resulting in a lift of the partial clinical hold. The start of the MRCLS trial was delayed as a result of the FDA issued partial clinical hold and there is no guarantee that any later MRCLS pivotal trial or further SPEAR T-cell trial will be approved by the FDA.
We are in the process of expanding our clinical trial foot print to Europe. This requires gaining approval of country specific review bodies for GMO application and CTA. As this is not a harmonized process, the requirements can vary considerably and delays can be incurred at a country level.
In the USA, some IRBs have requested that the Sponsor obtain Investigational Device Exemptions (IDE) from the FDA for the validated clinical trial assay being used to select patients. This has delayed the initiation of some sites and limited the ability to obtain high risk biopsies until an IDE has been granted. Adaptimmune plans to proactively seek IDE for our SPEAR T-cells where appropriate.
29
Table of Contents
Our SPEAR T-cells being developed may have potentially fatal cross-reactivity to other peptides or protein sequences within the body.
One of our prior SPEAR T-cells, designed to target an HLA-1 restricted MAGE-A3 cancer-specific peptide, recognized another unrelated peptide from a protein called TITIN, expressed within normal cardiac and other muscle tissues in patients. As a result of this cross-reactivity to the TITIN protein in the heart, two patients died during our MAGE-A3 clinical program, the program was put on pause, then formally placed on hold by the FDA, after which we terminated the program. We subsequently developed a preclinical safety testing program that identifies potential cross-reactivity risks but there may be gaps or other problems detected in the testing program at a later date. Even with the use of this testing program, there can be no guarantee that the FDA will permit us to begin clinical trials of any additional SPEAR T-cells other than those for which INDs already exist or that other off-target cross-reactivity will not be identified or present in any patient group. Failure to develop an effective preclinical safety testing program will prevent or delay clinical trials of any SPEAR T-cell. Detection of any cross-reactivity will halt or delay any ongoing clinical trials for any SPEAR T-cell and prevent or delay regulatory approval. Given that the underlying technology platform, manufacturing process and development process is similar for all of our TCR therapies, issues pertaining to cross-reactivity for one SPEAR T-cell may impact our ability to obtain regulatory approval for other SPEAR T-cells undergoing development and clinical trials, which would significantly harm our business, prospects, financial condition and results of operations.
Cross-reactivity or allo-reactivity (binding to peptides presented on other HLA types) could also occur where the affinity-enhanced engineered TCR resulting from administration of our SPEAR T-cell binds to peptides presented by HLAs other than the HLA type for which the relevant TCR was developed. We have developed a preclinical screening process to identify allo-reactivity risk. Where any allo-reactivity risk is identified, patients with the allo-reactive alleles will be excluded from the trial. Any allo-reactivity or other cross-reactivity that impacts patient safety could materially impact our ability to advance our SPEAR T-cells into clinical trials or to proceed to market approval and commercialization. In addition, there is no guarantee that exclusion of patients with the identified allo-reactive allele will successfully eliminate the risk of allo-reactivity, and serious side effects for patients may still exist. Given that the underlying technology platform, manufacturing process and development process are similar for all of our SPEAR T-cells, issues pertaining to allo-reactivity for one SPEAR T-cell may impact our ability to obtain regulatory approval for other SPEAR T-cells undergoing development and clinical trials, which would significantly harm our business, prospects, financial condition and results of operations.
Our T-cell therapy, which is a type of cell therapy that uses gene therapy technology, represents a novel approach to cancer treatment that could result in heightened regulatory scrutiny, delays in clinical development, or delays in or our inability to achieve regulatory approval or commercialization of our SPEAR T-cells.
Use of our SPEAR T-cells to treat a patient requires the use of gene therapy technology, which involves combining a patient’s T cells with our lentiviral delivery vector containing the gene for our affinity-enhanced engineered TCR. This is a novel treatment approach that carries inherent development risks. We are therefore constantly evaluating and adapting our SPEAR T-cells following the results obtained during development work and the clinical programs. Further development, characterization and evaluation may be required, depending on the results obtained, in particular where such results suggest any potential safety risk for patients. The need to develop further assays, or to modify in any way the protocols related to our SPEAR T-cells to improve safety or effectiveness, may delay the clinical program, regulatory approval or commercialization, if approved at all, of any SPEAR T-cell. Consequently, this may have a material impact on our ability to receive milestone payments and/or generate revenue from our SPEAR T-cells.
In addition, given the novelty of our SPEAR T-cells, the end users and medical personnel require a substantial amount of education and training in their administration of our SPEAR T-cells. Regulatory authorities have very limited experience with commercial engineered cell therapies and SPEAR T-cells for the treatment of cancer. As a result, regulators may be more risk adverse or require substantial dialogue and education as part of the normal regulatory approval process for each stage of development of any SPEAR T-cell. To date, only a limited number of gene therapy products have been approved in the United States and European Union. Consequently, it is difficult to predict and evaluate what additional regulatory hurdles may apply to the development of our SPEAR T-cells and whether additional investment, time or resources will be required to overcome any such hurdles.
Additionally, because our technology involves the genetic modification of patient cells ex-vivo using a viral vector, we are subject to many of the challenges and risks of gene therapy, including the following challenges:
· Regulatory requirements governing gene and cell therapy products have changed frequently and may continue to change in the future.
30
Table of Contents
· Random gene insertion associated with retrovirus-mediated genetically modified products, known as insertional oncogenesis, could lead to lymphoma, leukemia or other cancers, or other aberrantly functioning cells. Insertional oncogenesis was seen in early gene therapy studies conducted outside of the United States in 2003. In those studies, insertional oncogenesis resulted in patients developing leukemia following treatment with the relevant gene therapy, with one patient dying. As a result of the data from those studies, the FDA temporarily halted gene therapy trials in the United States. The previous trials involved modification of stem cells rather than T cells and utilized a murine gamma-retroviral vector rather than a lentiviral vector. We cannot guarantee that insertional oncogenesis resulting from administration of our SPEAR T-cells will not occur.
· Although our viral vectors are not able to replicate, there may be a risk with the use of retroviral or lentiviral vectors that they could undergo recombination and lead to new or reactivated pathogenic strains of virus or other infectious diseases.
· There is the potential for delayed adverse events following exposure to gene therapy products due to persistent biological activity of the genetic material or other components of products used to carry the genetic material. In part for this reason, the FDA recommends a 15-year follow-up observation period for all surviving patients who receive treatment using gene therapies in clinical trials. We may need to adopt such an observation period for our therapeutic candidates; however, the FDA does not require that the tracking be complete prior to its review of the BLA.
· Clinical trials using genetically modified cells conducted at institutions that receive funding for recombinant DNA research from the NIH may be subject to review by the NIH Office of Biotechnology Activities’ RAC. The RAC review process can delay or impede the initiation of a clinical trial. New guidelines were introduced by the NIH in April 2016 relating to the RAC review process for protocols using genetically modified cells and there is uncertainty as to how the new guidelines will operate. This could lead to increased delays in the approval of our protocols or additional education of institution review committees or boards being required during the protocol review process.
If adverse events of the type described above were to occur, further advancement of our clinical trials could be halted or delayed, which would have a material adverse effect on our business and operations. In addition, heightened regulatory scrutiny of gene therapy product candidates may result in delays and increased costs in bringing a product candidate to market, if at all. Delay or failure to obtain, or unexpected costs in obtaining, the regulatory approval necessary to bring a potential product to market could decrease our ability to generate revenue in the future.
In addition, results seen in third party clinical trials using other cell therapy products, for example CAR-T products, may impact on the further advancement of our clinical trials. For example, the deaths reported in a trial using a CAR-T directed against CD19 (JCAR-015) in adult patients with Adult Lymphoblastic Leukemia (ALL) (Juno Therapeutics, NCT02535364) may impact on our ability to further advance our clinical trials or result in the FDA requiring amendments or changes to the protocols used for our clinical trials. Based on the data currently available to us in relation to our clinical trials there is no evidence that the type and severity of neurotoxological events observed with CD19-directed CAR-T cell treatments, including the fatal events observed in the NCT02535364 trial, occur with Adaptimmune’s NY-ESO-1 TCRs and we do not therefore believe that any changes to our SPEAR T-cell clinical trial protocols are required. However there is no guarantee that the FDA or other regulatory authorities will agree with that position and further education and discussion with regulatory authorities may be required.
T-cell therapy is a novel approach to cancer treatment that creates significant increased risk in terms of side-effect profile, ability to satisfy regulatory requirements associated with clinical trials and the long- term viability of administered SPEAR T-cells.
Development of a pharmaceutical or biologic therapy or product has inherent risks based on differences in patient population and responses to therapy and treatment. The mechanism of action and impact on other systems and tissues within the human body following administration of our SPEAR T-cell is not completely understood, which means that we cannot predict the long-term effects of treatment with our SPEAR T-cells.
We are aware that certain patients do not respond to our SPEAR T-cells and that other patients may relapse or cease to present the peptide being targeted by such SPEAR T-cells. The percentage of the patient population in which these events may occur is unknown, but the inability of patients to respond and the possibility of relapse may impact our ability to conduct clinical trials, to obtain regulatory approvals, if at all, and to successfully commercialize any SPEAR T-cell.
Our clinical trials and the investigator-initiated clinical trials using our NY-ESO TCR therapeutic are still in the early stages, and it is difficult to predict the results that will be obtained in ongoing clinical trials or the next phase or phases of any clinical program. Our SPEAR T-cells have not previously been tested in combination clinical trials, for example use in combination with Merck’s PD-1 inhibitor, KEYTRUDA® (pembrolizumab) in patients with multiple myeloma. It is difficult to predict the way in which our SPEAR T-cells will interact with third-party products used in combination clinical trials. Any undesirable side effects seen in combination trials may affect our ability to continue with and obtain regulatory approval for the combination therapy, but may also impact our ability to continue with and obtain regulatory approval for our SPEAR T-cell therapies alone.
31
Table of Contents
There is a significant risk at each stage of any clinical program that serious adverse events or low efficacy, as well as less favorable benefit:risk profiles, will prevent our SPEAR T-cells from proceeding further or will result in those programs being suspended or placed on hold (whether voluntarily or as a result of a regulatory authority requirement). For example, there is a risk that the target (or similar) peptide to which any SPEAR T-cell is directed may be present in both patients’ cancer cells and other non-cancer cells and tissues. Should this be the case patients may suffer a range of side effects associated with the SPEAR T-cell binding to both the cancer cells and/or other cells and tissues and such side effects could cause patient death. The extent of these side effects will depend on which cells and tissues are affected as well as the degree to which the target (or similar) peptide is expressed in these cells and tissues.
As of January 5, 2017, 61 subjects have received NY-ESO SPEAR T-cells in Adaptimmune-sponsored studies. The most common (>15%) adverse events in these subjects considered by investigators to be at least possibly related to our NY-ESO SPEAR T-cells include: fever, diarrhea, fatigue, rash, nausea, anemia, dyspnea, CRS, lymphopenia, leukopenia, cough, ALT increased, AST increased, hypotension, sinus tachycardia, neutropenia, and thrombocytopenia. Adverse events with severity grade 3 or higher considered by investigators to be at least possibly related and occurring in more than one patient include lymphopenia, leukopenia, anemia, neutropenia, febrile neutropenia, diarrhea, CRS, graft versus host disease, hyponatremia, and musculoskeletal chest pain. There has been one report of fatal (grade 5) treatment related to bone marrow failure which was considered related to study treatment by the investigator in the trial. Internal investigations have not identified a mechanism by which NY-ESO SPEAR T-cells may have caused bone marrow failure. Serious adverse events (SAEs) have also been reported on our Company sponsored clinical programs. SAEs considered by investigators to be at least possibly related and occurring in more than one patient include: fever, cytokine release syndrome, dehydration, graft versus host disease, neutropenia, and rash. To date, GVHD, impacting the skin and gastrointestinal tract, has only been reported in our myeloma study involving autologous stem cell transplants (ASCT). Although GVHD is a known complication of ASCT, symptoms such as rash, colitis and diarrhea have been reported in other NY-ESO SPEAR T-cell studies. There have also been reports of serious unexpected adverse reactions considered at least possibly related by investigators in our trials: grade 2 rhabdomyolysis possibly due to breakdown of a myeloma plasmacytoma that was thought to be infiltrating the muscle tissue based on a CT scan; grade 3 dehydration requiring overnight hospital admission; grade 4 supraventricular tachycardia (SVT) in one patient and grade 4 respiratory failure with grade 4 febrile neutropenia in a second patient (this patient recovered from respiratory failure and febrile neutropenia but later experienced fatal bone marrow failure); one case of pre-existing pericardial effusion has been reported and recently there have been reports of a grade 3 thromboembolic event, grade 2 pneumonitis, and grade 2 tumor related chest pain.
In our ovarian cancer trial with our NY-ESO SPEAR T-cell, the first patient treated experienced a grade 3 cytokine release syndrome at day seven post-infusion, concomitant with a significant proliferation of the engineered T-cells that constituted the majority of the peripheral white blood cells at day 14. This level of cytokine release syndrome had not been seen in previous results from trials using our NY-ESO SPEAR T-cell. The patient’s tumor markers were also falling during this time. To manage the cytokine release syndrome, the patient was treated with high dose steroids that likely abrogated the engineered T-cell function. All Adaptimmune protocols now allow for use of the anti-IL6R antibody, tocilizumab, for treatment of cytokine release syndrome in future patients. Tocilizumab has been shown to control cytokine release syndrome likely without abrogating the anti-tumor response.
In addition to our Company sponsored clinical programs, our NY-ESO TCR therapeutic has also been used in an investigator-initiated clinical program funded by the European Union, referred to as the ATTACK 2 program. The therapy, which was produced under a different manufacturing process than Adaptimmune’s NY-ESO TCR therapy, was being evaluated for the treatment of patients with advanced gastro-esophageal cancer for the first time. To date, two patients have been treated under this protocol, one of whom passed away 46 days after initial treatment. Said patient experienced enterocolitis and bone marrow failure followed by fatal gangrenous gastrointestinal necrosis and hemorrhage. The investigator determined there was a reasonable possibility that these events were caused by study treatment.
Enrollment in the trial was temporarily paused pending investigation of the patient fatality, but an independent data monitoring committee has since recommended that recruitment can resume following a protocol amendment. The European Union has since terminated funding of the trial due to the delays in trial progression and the Company is in discussions with the sponsor, the Christie NHS Trust, in relation to any continuation of the trial. The enrollment of patients in our own sponsored clinical trials using our NY-ESO SPEAR T-cells have not been affected so far, although regulatory authorities in the United Kingdom and United States were informed of the event. If and when recruitment re-starts in the ATTACK 2 program, if any safety risk to patients is identified which is potentially associated with our NY-ESO SPEAR T-cell, our Company sponsored clinical trials could be affected, including the possibility of being placed on hold.
32
Table of Contents
Because administration of our SPEAR T-cells is patient-specific, the process requires careful handling of patient-specific products and fail-safe tracking, namely the need to ensure that the tracking process is without error and that patient samples are tracked from patient removal, through manufacturing and re-administration to the same patient. We will need to invest in systems, such as bar coding, to ensure fail safe tracking. There is always a risk of a failure in any such system. Inability to develop or adopt an acceptable fail-safe tracking methodology and handling regime may delay or prevent us from receiving regulatory approval. This risk may be increased where our SPEAR T-cells are used in clinical programs that we do not control or sponsor and, should an error be made in the administration of our SPEAR T-cells in such clinical programs, this could affect the steps required in our own clinical programs and manufacturing process requiring the addition of further tracking mechanisms to ensure fail-safe tracking. The tracking systems required to ensure safe patient administration may also require increased administration to satisfy other regulatory requirements, for example data protection requirements in Europe. The need to ensure tracking systems are adequate and to comply with these additional regulatory requirements may result in delay to the start of trials or the need to obtain additional regulatory licenses or consents prior to starting such trials.
Validation of our SPEAR T-cells requires access to human samples but there is no guarantee that such samples can be obtained or, if they can be obtained, that the terms under which they are provided will be favorable to us.
Certain of the steps involved in validating and carrying out safety testing in relation to our SPEAR T-cells require access to samples (e.g., tissues samples or cell samples) from third parties. Such samples may be obtained from universities or research institutions and will often be provided, subject to satisfaction of certain terms and conditions. There can be no guarantee that we will be able to obtain samples in sufficient quantities to enable development of and use of the full preclinical safety testing program for all SPEAR T-cells undergoing development. In addition, the terms under which such samples are available may not be acceptable to us or may restrict our use of any generated results or require us to make payments to the third parties.
Our SPEAR T-cells and their application are not fully scientifically understood and are still undergoing validation and investigation.
Our SPEAR T-cells and their potential associated risks are still under investigation. For example, there is a potential risk that, given that the TCR chains are produced separately and then assembled within patient T cells into full TCRs, the TCR chains from both transduced and naturally occurring T cells could be assembled into an unintended end TCR due to mis-pairing of TCR chains, which could create unknown recognition and cross-reactivity problems within patients. Although this phenomenon has not been reported in humans, it remains a theoretical risk for our SPEAR T-cells and is still being studied and investigated. This could delay regulatory approval, if any, for the relevant SPEAR T-cells. To the extent that any mis-pairing of TCR chains is identified, either in our or our competitors’ clinical trials, additional investment may be required in order to modify relevant SPEAR T-cells and to further assess and validate the risk of such mis-pairing to patients. There is also no guarantee that following modification of the relevant SPEAR T-cell, such modified SPEAR T-cell will remain suitable for patient treatment, that it will eliminate the risk of mis-pairing of TCR chains or that regulatory approval will be obtained at all or on a timely basis in relation to such modified SPEAR T-cells. The occurrence of such events could significantly harm our business, prospects, financial condition and results of operations.
We may not be able to identify and validate additional target peptides or isolate and develop affinity-enhanced TCRs that are suitable for validation and further development.
The success of our SPEAR T-cells depends on both the identification of target peptides presented on cancer cells, which can be bound by TCRs, and isolation and affinity enhancement of TCRs, which can be used to treat patients if regulatory approval is obtained. There is an inherent risk that the number of target peptides that can be identified and/or our ability to develop and isolate suitable TCRs for affinity enhancement could be significantly lower than projected or that no additional SPEAR T-cells suitable for further development can be identified. Any failure to identify and validate further target peptides will reduce the number of potential SPEAR T-cells that we can successfully develop, which in turn will reduce the commercial opportunities available to us and increase our reliance on our existing SPEAR T-cells.
In addition, there is no guarantee that our attempts to develop further SPEAR T-cells will result in candidates for which the safety and efficacy profiles enable progression to and through preclinical testing. Failure to identify further candidates for progression into preclinical testing and clinical programs will significantly impact our commercial returns, increase our reliance on the success of our existing SPEAR T-cell programs and may significantly harm our business, prospects, financial condition and results of operations. If resources become limited or if we fail to identify suitable target peptides, TCRs or affinity-enhanced TCRs, our ability to submit INDs for further SPEAR T-cells may be delayed or never realized, which would have a materially adverse effect on our business.
33
Table of Contents
We may encounter substantial delays in our clinical trials or may not be able to conduct our trials on the timelines we expect.
Conduct of clinical trials is dependent on finding clinical sites prepared to carry out the relevant clinical trials, screening of patients by the clinical sites, recruitment of patients both in terms of number and type of patients and general performance of the relevant clinical site. It is difficult to predict how quickly we will be able to recruit suitable patients, find suitable sites, begin clinical programs and administer our SPEAR T-cells. The patient population in which any required peptide antigen is presented may be lower than expected which will increase the timescales required to find and recruit patients into the applicable clinical trial. Screening of a large number of patients is required to identify HLA and tumor antigen positive patients for most of our clinical trials. For example it has taken longer to recruit patients into our NSCLC trials with both our NY-ESO SPEAR T-cell and MAGE-A10 SPEAR T-cell due to the low percentage expression of peptide antigen seen in the patient populations at the relevant clinical trial sites. With our NY-ESO SPEAR T-cell, presentation of the antigen occurs predominantly in certain sub-types of NSCLC and additional clinical sites may need to be initiated in order to identify patients with those certain NSCLC sub-types. With MAGE-A10 presentation of the peptide antigen is seen in a lower number of patients than anticipated. This will delay recruitment of patients into NSCLC trials for both therapies and result in the Company incurring additional costs associated with the need to find and initiate additional clinical trial sites. It is also difficult to predict whether changes may be required to any clinical trial design as our clinical trials progress. For example, initial results from current Phase 1/2 clinical trials with our NY-ESO SPEAR T-cell have suggested that fludarabine is required as part of any patient pre-conditioning regimen. This has required amendment to protocol designs, which did not previously include fludarabine, to include fludarabine.
Our clinical trials will compete with other clinical trials that are in the same therapeutic areas as our SPEAR T-cells, which will reduce the number and types of patients available to us, because some patients who might have opted to enroll in our trials may instead opt to enroll in a trial being conducted by one of our competitors. Because the number of qualified clinical investigators is limited, we will conduct some of our clinical trials at the same clinical trial sites that some of our competitors use, which will reduce the number of patients who are available for our clinical trials at such clinical trial sites. Moreover, because our SPEAR T-cells represent a departure from more commonly used methods for cancer treatment, potential patients and their physicians may opt to use conventional therapies, such as chemotherapy and hematopoietic cell transplantation, rather than enrollment in any of our current or future clinical trials. In addition, in relation to any indication, the standard of care for patients in that indication may change or further develop meaning that clinical sites are no longer prepared to continue with any clinical trial or require amendments to agreed protocols for clinical trials. For example, the standard of care in melanoma has changed since the start of our clinical trials in melanoma with our NY-ESO SPEAR T-cell and as a result the clinical trial has been halted due to anticipated unavailability of patients. Such circumstances can lead to the suspension of the relevant clinical trial at a site, inability to recruit further patients at that clinical site or a requirement to amend the protocol, all of which will delay or potentially halt progression of a SPEAR T-cell through clinical trials.
Even if we are able to enroll a sufficient number of patients in our clinical trials, delays in patient enrollment may result in increased costs or may affect the timing or outcome of the planned clinical trials, which could prevent completion of these trials and adversely affect our ability to advance the development of our SPEAR T-cells.
Our synovial sarcoma pivotal trial start date relies on approval of comparability studies related to the manufacturing of our SPEAR T-cells. If the results from the comparability studies are not acceptable, this may delay the start of the synovial sarcoma pivotal trial and require re-evaluation of the process used to manufacture of our SPEAR T-cells.
We may not be able to develop or obtain approval for the analytical assays and companion diagnostics required for commercialization of our SPEAR T-cells.
Administration of our SPEAR T-cells requires the use of an immuno-chemistry or other screening assay in which patients are screened for the presence of the cancer peptide targeted by our SPEAR T-cells. This assay requires the identification of suitable antibodies which can be used to identify the presence of the relevant target cancer peptide.
If safe and effective use of a biologic product depends on an in vitro diagnostic, such as a test to detect patients with HLA type A2, then the FDA generally requires approval or clearance of the diagnostic, known as a companion diagnostic, concurrently with approval of the therapeutic product. To date, the FDA has generally required in vitro companion diagnostics that are intended for use in selection of patients who will respond to cancer treatment to obtain a pre-market approval, or PMA, which can take up to several years, for that diagnostic simultaneously with approval of the biologic product.
We expect that, for our NY-ESO SPEAR T-cell, the FDA and similar regulatory authorities outside of the United States will require the development and regulatory approval of a companion diagnostic assay as a condition to approval. We also expect that the FDA may require PMA supplemental approvals for use of that same companion diagnostic as a condition of approval of additional SPEAR T-cells. We do not have experience or capabilities in developing or commercializing these companion diagnostics and plan to rely in large part on third parties to perform these functions.
34
Table of Contents
If we, or any third parties that we engage to assist us, are unable to successfully develop companion diagnostic assays for use with our SPEAR T-cells, or are unable to obtain regulatory approval or experience delays in either development or obtaining regulatory approval, we may be unable to identify patients with the specific profile targeted by our SPEAR T-cells for enrollment in our clinical trials. Accordingly, further investment may be required to further develop or obtain the required regulatory approval for the relevant companion diagnostic assay, which would delay or substantially impact our ability to conduct further clinical trials or obtain regulatory approval.
Manufacturing and administering our SPEAR T-cells is complex and we may encounter difficulties in production, particularly with respect to process development or scaling up of our manufacturing capabilities. If we encounter such difficulties, our ability to provide supply of our SPEAR T-cells for clinical trials or for commercial purposes could be delayed or stopped.
The process of manufacturing and administering our SPEAR T-cells is complex and highly regulated. The manufacture of our SPEAR T-cells involves complex processes, including manufacture of a lentiviral delivery vector containing the gene for our affinity-enhanced engineered TCR. Administration of our SPEAR T-cells includes harvesting white blood cells from the patient, isolating certain T cells from the white blood cells, combining patient T cells with our lentiviral delivery vector through a process known as transduction, expanding the transduced T cells to obtain the desired dose, and ultimately infusing the modified T cells back into the patient. As a result of the complexities, our manufacturing and supply costs are likely to be higher than those at more traditional manufacturing processes and the manufacturing process is less reliable and more difficult to reproduce. Our manufacturing process is and will be susceptible to product loss or failure due to logistical issues, including manufacturing issues associated with the differences in patients’ white blood cells, interruptions in the manufacturing process, contamination, equipment or reagent failure, supplier error and variability in SPEAR T-cell and patient characteristics.
For example, to manufacture our lentiviral delivery vector manufacturing slots have to be agreed in advance with third party contract manufacturers. It has not always been possible to obtain manufacturing slots within the timescales we require for supply of lentiviral delivery vector or to obtain agreed dates for such manufacturing slots sufficiently in advance of the requirement for supply. In addition third party contract manufacturers have cancelled or delayed the start of manufacturing slots, even where such manufacturing slots have been pre-agreed. This has necessitated the use of additional third party contract manufacturers. We cannot guarantee that manufacturing slots will be available within the timescales we require for ongoing supply of SPEAR T-cells. In relation to ongoing NY-ESO SPEAR T-cell trials, this may result in delays in supply of the lentiviral delivery vector and has required us to source alternative third party contract manufacturers for supply of the lentiviral delivery vector. In relation to new clinical trials, cancellation and delay in the start of manufacturing slots may result and has resulted, in the case of our AFP SPEAR T-cell, in delay in the start of or enrollment of patients into our clinical trials.
If for any reason we (or any other manufacturer of our therapy) lose a patient’s white blood cells or such material gets contaminated or later processing steps fail at any point, the manufacturing process of the SPEAR T-cell for that patient will need to be completely restarted and the resulting delay may adversely affect that patient’s outcome. If microbial, viral or other contaminations are discovered in our SPEAR T-cells or in the manufacturing facilities in which our SPEAR T-cells are made or administered, such manufacturing facilities may need to be closed for an extended period of time to investigate and remedy the contamination.
The requirements for manufacture and supply of SPEAR T-cells for clinical trials in Europe have additional complexities and the manufacture and supply of our SPEAR T-cells is raising issues which have not previously been regulated or observed by the relevant regulatory authorities. For example, supply of SPEAR T-cells for European clinical trials will either require manufacture of SPEAR T-cells in the United States or use of a new CMO in Europe. Where manufacture continues in the United States, there is a need to transfer patient product from clinical sites in Europe to the manufacturer in the United States, for the patient product to be converted into our end SPEAR T-cell product and then for that SPEAR T-cell product to be transported back to the site in Europe for administration to the patient. The supply and manufacturing chain required to achieve this is very complex and could be subject to failures at any point in the supply and manufacturing chain. We are in the process of transferring the manufacturing process to a third-party manufacturer in Europe, but the third-party manufacturer is as yet untested and has not previously supplied any of our SPEAR T-cell product. Any inability to set up acceptable manufacturing and supply chains to enable treatment of patients in Europe could result in delay to those trials starting in Europe.
35
Table of Contents
As our SPEAR T-cells progress through preclinical programs and clinical trials towards approval and commercialization, it is expected that various aspects of the manufacturing and administration process will be altered in an effort to optimize processes and results. We have already identified some improvements to our manufacturing and administration processes, but these changes may not achieve the intended objectives, may not be transferable to third parties or able to be used at larger scales and could cause our SPEAR T-cells to perform differently or affect the results of planned clinical trials or other future clinical trials. In addition, such changes may require amendments to be made to regulatory applications or comparability tests to be conducted which may further delay the timeframes under which modified manufacturing processes can be used for any SPEAR T-cell. For example, we are planning to make changes to the manufacturing process for cell products and vector material used in our NY-ESO SPEAR T-cell for which we will need to conduct clinical trials to gather safety data for each of the different indications for which larger clinical trials are planned. If our NY-ESO SPEAR T-cell manufactured under the new process has a worse safety or efficacy profile than the prior investigational product, we may need to re-evaluate the use of that manufacturing process, which could significantly delay or even result in the halting of our clinical trials.
Developing a commercially viable process is a difficult and uncertain task, and there are risks associated with scaling to the level required for advanced clinical trials or commercialization, including, among others, increased costs, potential problems with process scale-out, process reproducibility, stability issues, lot consistency, loss of product, and timely availability of reagents or raw materials or contract manufacturing services or facilities. A failure to develop such a commercially viable process within anticipated timescales may prevent or delay progression of our T-cell therapies into pivotal clinical trials and ultimately commercialization. In addition, we may ultimately be unable to reduce the expenses associated with our SPEAR T-cells to levels that will allow us to achieve a profitable return on investment.
We are in the process of developing and transferring new processes to facilitate such manufacture into third-party contract suppliers. Any delay in the development and transfer of these new processes to the third-party contract supplier or inability of the third-party contract supplier to replicate or carry out the transferred process at the appropriate level and quality will result in delays in our ability to progress clinical programs, further develop our SPEAR T-cells and obtain marketing approval for our SPEAR T-cells. Such process scale-up and transfer will also require a demonstration of comparability between the product used in clinical trials and the potential commercial product manufactured by the new process at the new facility. If we are unable to demonstrate that our commercial scale product is comparable to the product used in clinical trials, or the regulatory authority requires additional comparability testing to be carried out, we may not receive regulatory approval for that product without additional clinical trials. We cannot guarantee that we will be able to make the required modifications or perform the required comparability testing within currently anticipated timeframes or that such modifications or comparability testing, when made, will obtain regulatory approval or that the new processes or modified processes will successfully be transferred to the third party contract suppliers within currently anticipated timeframes.
Transfer of our new process for manufacture of the lentiviral vector used to manufacture our NY-ESO SPEAR T-cells to our third party contract manufacturing organization (“CMO”) has taken substantially longer than originally predicted and there is no guarantee that such technology will be successfully transferred to such third party CMO in the near term or at all. If such transfer is not possible or fails to generate the required levels of product we may need to source alternative CMOs. Any delay, whether in end T-cell product or vector product will also impact when clinical trials may start. Such failure may also impact our collaboration with GSK and result in GSK not exercising options or not developing any of our additional SPEAR T-cells. Even if we are successful, our manufacturing capabilities could be affected by increased costs, unexpected delays, equipment failures, labor shortages, natural disasters, power failures and numerous other factors that could prevent us from realizing the intended benefits of our manufacturing strategy, which in turn could have a material adverse effect on our business.
We have insurance to cover certain business interruption events, particularly research and development expenditure (capped at £10 million) and committed costs (capped at £250,000). However, because our level of insurance is capped, it may be insufficient to fully compensate us if any of these events were to occur in the future.
36
Table of Contents
Our manufacturing process needs to comply with FDA regulations and foreign regulations relating to the quality and reliability of such processes. Any failure to comply with relevant regulations could result in delays in or termination of our clinical programs and suspension or withdrawal of any regulatory approvals.
In order to commercially produce our products, we will need to comply with the FDA’s cGMP requirements. Such compliance requirements will also apply to any manufacture of SPEAR T-cells at our Navy Yard manufacturing facility, once operational. We may encounter difficulties in achieving quality control and quality assurance and may experience shortages in qualified personnel. We and our third party contract manufacturers are subject to inspections by the FDA and comparable agencies in other jurisdictions to confirm compliance with applicable regulatory requirements once the process has been approved. Any failure to follow cGMP or other regulatory requirements or delay, interruption or other issues that arise in the manufacture, fill- finish, packaging, or storage of our SPEAR T-cells as a result of a failure of our facilities or the facilities or operations of third parties to comply with regulatory requirements or pass any regulatory authority inspection could significantly impair our ability to develop and commercialize our SPEAR T-cells, including leading to significant delays in the availability of our SPEAR T-cells for our clinical trials or the termination of or suspension of a clinical trial, or the delay or prevention of a filing or approval of marketing applications for our SPEAR T-cells. Significant non-compliance could also result in the imposition of sanctions, including warning letters, fines, injunctions, civil penalties, failure of regulatory authorities to grant marketing approvals for our SPEAR T-cells, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of products, operating restrictions and criminal prosecutions, any of which could damage our reputation and our business.
When we start manufacturing our SPEAR T-cells at our own facility, there is no guarantee that we will be able to comply with the FDA’s cGMP requirements or the requirements of other regulatory authorities either at all or within anticipated timescales. In addition, once our manufacturing facility is up and running there is no guarantee that any SPEAR T-cells produced in such facility will be able to meet regulatory requirements or that we will be able to recruit sufficient staff to enable manufacture of products within required timescales. Any failure to meet regulatory requirements or produce SPEAR T-cells according to regulatory requirements could result in delays to our clinical programs and may result in withdrawal of regulatory approval for our manufacturing facility.
The outcome of clinical trials is uncertain and our clinical trials may fail to demonstrate adequately the safety and efficacy of any of our SPEAR T-cells which would prevent or delay regulatory approval and commercialization.
There is a risk in any clinical trial (whether sponsored by us or investigator-initiated) that side effects from our SPEAR T-cells will require a hold on, or termination of, our clinical programs or further adjustments to our clinical programs in order to progress our SPEAR T-cell. Our SPEAR T-cells are novel and unproven and regulators will therefore require evidence that the SPEAR T-cells are safe before permitting clinical trials to commence and evidence that the SPEAR T-cells are safe and effective before granting any regulatory approval. In particular, because our SPEAR T-cells are subject to regulation as biological products, we will need to demonstrate that they are safe, pure and potent for use in each target indication. The SPEAR T-cell must demonstrate an acceptable benefit:risk profile in its intended patient population and for its intended use. The benefit:risk profile required for product licensure will vary depending on these factors and may include not only the ability to show tumor shrinkage, but also adequate duration of response, a delay in the progression of the disease and/or an improvement in survival. For example, response rates from the use of our SPEAR T-cells will not be sufficient to obtain regulatory approval unless we can also show an adequate duration of response. The FDA previously issued a partial clinical hold for the Company’s MRCLS trial with NY-ESO following review of the IND submitted for the trial. This partial clinical hold has now been lifted. However, there can be no guarantee that the FDA or other regulatory authorities will not issue further clinical holds in relation to the MRCLS trial or other trials.
The regulatory authorities (including the FDA) may issue a hold on our clinical trials as a result of safety information and data obtained in third party clinical trials. For example the deaths reported in a trial using a CAR-T directed against CD19 (JCAR-015) in adult patients with Adult Lymphoblastic Leukemia (ALL) (Juno Therapeutics, NCT02535364) may impact on our ability to further advance our clinical trials with clinical sites or result in the FDA requiring amendments or changes to the protocols used for our clinical trials. Based on the data currently available to us in relation to our clinical trials there is no evidence that the neurotoxicity observed with CD19-directed CAR-T cell treatments, including the fatal events observed in the NCT02535364 trial occur with Adaptimmune’s NY-ESO-1 TCRs and we do not therefore believe that any changes to our SPEAR T-cell clinical trial protocols are required. However, there is no guarantee that the FDA or other regulatory authorities will agree with that position and further education and discussion with regulatory authorities may be required. Any such hold will require addressing by the Company and will inevitably delay progression of the clinical trials concerned, if such clinical trials progress at all.
37
Table of Contents
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. Success in preclinical programs and early clinical trials does not ensure that later clinical trials will be successful. For example, our SPEAR T-cells have only been used in Phase 1/2 clinical trials to date and the extent to which our SPEAR T-cells will continue to persist in patients and, if they do persist, continue to have an effect in patients is currently unknown. Moreover, the results of preclinical programs and early clinical trials of our SPEAR T-cells may not be predictive of the results of later-stage clinical trials. To date, we have only obtained interim results from Phase 1/2 clinical trials that are uncontrolled, involve small sample sizes and are of shorter duration than might be required for regulatory approval. There may be other reasons why our early clinical trials are not predictive of later clinical trials. In addition, the results of trials in one set of patients or line of treatment may not be predictive of those obtained in another and protocols may need to be revised based on unexpected early results. For example, in our ovarian cancer trial with our NY-ESO SPEAR T-cell, the first patient treated experienced a grade 3 cytokine release syndrome at day seven post-infusion, concomitant with a significant proliferation of the engineered T cells that constituted nearly 100% of the peripheral blood at day 14. This level of cytokine release syndrome had not been seen in previous results from trials using our NY-ESO SPEAR T-cell. The patient’s tumor markers were also falling during this time. To manage the cytokine release syndrome, the patient was treated with high dose steroids that likely abrogated the engineered T-cell function. The protocol was then modified to allow for use of the anti-IL6R antibody, tocilizumab, for treatment of cytokine release syndrome in future patients, which has been shown to control cytokine release syndrome likely without abrogating the anti-tumor response. As another example, in both the European investigator-initiated clinical program in gastro-esophageal cancer and in our own sponsored synovial sarcoma trial there has been one patient death considered to be related to treatment according to the investigator.
We expect there may be greater variability in results for our SPEAR T-cells which are administered on a patient-by-patient basis than for “off-the-shelf” products, like many other biologics. There is typically an extremely high rate of attrition from the failure of any products proceeding through clinical trials. SPEAR T-cells in later stages of clinical trials may fail to show the desired safety and efficacy profile despite having progressed through preclinical programs and initial clinical trials. A number of companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or unacceptable safety issues, notwithstanding promising results in earlier trials. Most biologic candidates that begin clinical trials are never approved by regulatory authorities for commercialization. We cannot therefore guarantee that we will be successful in obtaining the required efficacy and safety profile from the performance of any of our clinical programs.
Certain of our clinical trials include dose escalation studies in which the dose of SPEAR T-cells administered to patients is varied or initial studies in which the pre-treatment regimen may be varied, for example a regimen with and without fludarabine. The outcome of such dose escalation or initial studies will inform the clinical study going forward. However, the need to carry out dose escalation or other initial studies may result in delays in data from such clinical programs while the most suitable dose or regimen is assessed. For example, the trial design for our MAGE-A4 and AFP trials includes dose escalation and therefore efficacy data may not be obtained from initial patients treated in such studies.
In addition, even if such trials are successfully completed, we cannot guarantee that the FDA or foreign regulatory authorities will interpret the results as we do. Accordingly, more trials may be required before we can submit our SPEAR T-cell for regulatory approval. To the extent that the results of the trials are not satisfactory to the FDA or foreign regulatory authorities for support of a marketing application, we may be required to expend significant resources, which may not be available to us, to conduct additional trials in support of potential approval of our SPEAR T-cells. We cannot predict whether any of our SPEAR T-cells will satisfy regulatory requirements at all or for indications in which such SPEAR T-cells are currently being evaluated as part of any clinical programs.
We have limited experience conducting clinical trials which may cause a delay in any clinical program and in the obtaining of regulatory approvals.
Although we have recruited a team that has significant experience with clinical trials, as a company we have limited experience in conducting clinical trials and no experience in conducting clinical trials through to regulatory approval. In part because of this lack of experience, we cannot be certain that planned clinical trials will begin or be completed on time, if at all. Large-scale trials would require significant additional financial and management resources, and reliance on third-party clinical investigators, contract research organizations, or CROs, or consultants. Relying on third-party clinical investigators, consultants or CROs may force us to encounter delays that are outside of our control.
Our SPEAR T-cells may have undesirable side effects or have other properties that could halt their clinical development, prevent their regulatory approval, limit their commercial potential or otherwise result in significant negative consequences.
Where any SPEAR T-cell has undesirable side effects, regulatory approval for such therapeutic may be delayed or suspended, or alternatively may be restricted to particular disease indications or states that are more limited than desirable. This could result in the failure of our products reaching the market or a reduction in the patient population for which any SPEAR T-cell can be used.
38
Table of Contents
As of January 5, 2017, 61 subjects have received NY-ESO SPEAR T-cells in Adaptimmune-sponsored studies. The most common (>15%) adverse events in these subjects considered by investigators to be at least possibly related to our NY-ESO SPEAR T-cells include: fever, diarrhea, fatigue, rash, nausea, anemia, dyspnea, CRS, lymphopenia, leukopenia, cough, ALT increased, AST increased, hypotension, sinus tachycardia, neutropenia, and thrombocytopenia. Adverse events with severity grade 3 or higher considered by investigators to be at least possibly related and occurring in more than one patient include lymphopenia, leukopenia, anemia, neutropenia, febrile neutropenia, diarrhea, CRS, graft versus host disease, hyponatremia, and musculoskeletal chest pain. There has been one report of fatal (grade 5) treatment related to bone marrow failure which was considered related to study treatment by the investigator in the trial. Internal investigations have not identified a mechanism by which NY-ESO SPEAR T-cells may have caused bone marrow failure. Serious adverse events (SAEs) have also been reported on our Company sponsored clinical programs. SAEs considered by investigators to be at least possibly related and occurring in more than one patient include: fever, cytokine release syndrome, dehydration, graft versus host disease, neutropenia, and rash. To date, GVHD, impacting the skin and gastrointestinal tract, has only been reported in our myeloma study involving autologous stem cell transplants (ASCT). Although GVHD is a known complication of ASCT, symptoms such as rash, colitis and diarrhea have been reported in other NY-ESO SPEAR T-cell studies. There have also been reports of serious unexpected adverse reactions considered at least possibly related by investigators in our trials: grade 2 rhabdomyolysis possibly due to breakdown of a myeloma plasmacytoma that was thought to be infiltrating the muscle tissue based on a CT scan; grade 3 dehydration requiring overnight hospital admission; grade 4 supraventricular tachycardia (SVT) in one patient and grade 4 respiratory failure with grade 4 febrile neutropenia in a second patient (this patient recovered from respiratory failure and febrile neutropenia but later experienced fatal bone marrow failure); one case of pre-existing pericardial effusion has been reported and recently there have been reports of a grade 3 thromboembolic event, grade 2 pneumonitis, and grade 2 tumor related chest pain.
In our NY-ESO SPEAR T-cell trials, CRS has been reported in 13/61 subjects who received NY-ESO SPEAR T-cells as of 02 January 2017. Of these 13 subjects, five subjects have experienced CRS at either Grade 3 or 4 in severity. There have been no reports of severe neurologic effects of CRS and no fatal CRS events. Subjects with more severe symptoms have generally responded to treatment with the anti-IL6R antibody, tocilizumab. All Adaptimmune protocols now allow for use of tocilizumab for treatment of cytokine release syndrome. Tocilizumab has been shown to control cytokine release syndrome likely without abrogating the anti-tumor response.
In addition to our Company sponsored clinical programs, our NY-ESO TCR therapeutic has also been used in an investigator-initiated clinical program funded by the European Union, referred to as the ATTACK 2 (Adoptive engineered T-cell Targeting to Activate Cancer Killing) program. The therapy, which was produced under a different manufacturing process than Adaptimmune’s NY-ESO TCR therapy, was being evaluated for the treatment of patients with advanced gastro-esophageal cancer for the first time. To date, two patients have been treated under this protocol, one of whom passed away 46 days after initial treatment. Said patient experienced enterocolitis and bone marrow failure followed by fatal gangrenous gastrointestinal necrosis and hemorrhage. The investigator determined there was a reasonable possibility that these events were caused by study treatment. Enrollment in the trial was temporarily paused pending investigation of the patient fatality but an independent data monitoring committee has since recommended that recruitment can resume following a protocol amendment. The European Union has since terminated funding of the trial due to the delays in trial progression and the Company is in discussions with the sponsor, the Christie NHS Trust, in relation to continuation of the trial. The trial is not enrolling patients whilst these discussions continue. The enrollment of patients in our own sponsored clinical trials using our NY-ESO SPEAR T-cells have not been affected so far, although regulatory authorities in the United Kingdom and United States were informed of the event. If and when recruitment re-starts in this program, if any safety risk to patients is identified which is potentially associated with our NY-ESO SPEAR T-cell, our Company sponsored clinical trials could be affected, including the possibility of being placed on hold.
Any unacceptable toxicities arising in ongoing clinical programs could result in suspension or termination of those clinical programs. Any suspension or termination may affect other SPEAR T-cells and thereby impact our ability to recognize any product revenues. Any side effects may also result in the need to perform additional trials, which will delay regulatory approval for such SPEAR T-cell, if at all, and require additional resources and financial investment to bring the relevant SPEAR T-cell to market.
In addition, the impact of SPEAR T-cells may vary from patient to patient and this may affect the number of patients who can be successfully treated with our SPEAR T-cells. Depending on the nature of the indication, certain patients may need to be excluded from treatment, which could also impact our ability to recruit patients to utilize such therapies or to recruit patients to conduct clinical trials in general for our SPEAR T-cells.
Use of our SPEAR T-cells in combination with other third party products or therapies, for example use in combination with Merck’s PD-1 inhibitor, KEYTRUDA® (pembrolizumab) in patients with multiple myeloma may increase or exacerbate side effects that have been seen with our SPEAR T-cells alone or may result in new side effects that have not previously been identified with our SPEAR T-cells alone. Our SPEAR T-cells have not previously been used in any combination clinical trials. Any undesirable side effects seen in combination trials may affect our ability to continue with and obtain regulatory approval for the combination therapy, but may also impact our ability to continue with and obtain regulatory approval for our SPEAR T-cell therapies alone.
39
Table of Contents
Clinical trials are expensive, time-consuming and difficult to implement.
Clinical trials, depending on the stage, can be costly as well as difficult to implement and define, particularly with technologies that are not tried and tested, such as our SPEAR T-cells. These factors can lead to a longer clinical development timeline and regulatory approval process, including a requirement to conduct further or more complex clinical trials in order to obtain regulatory approval. Regulatory authorities may disagree with the design of any clinical program, and designing an acceptable program could lead to increased timeframes for obtaining of approvals, if any. In addition, progression of clinical trials depends on the ability to recruit suitable patients to those trials and delay in recruiting will impact the timeframes of such clinical trials and as a result the timeframes for obtaining regulatory approval, if any, for the relevant SPEAR T-cells.
In particular, eligible patients must be screened for the target peptide and HLA type, which may reduce the number of patients who can be recruited for any clinical program. For example lower than expected patient numbers have been seen in the Company’s NSCLC clinical trials with its NY-ESO SPEAR T-cell and MAGE-A10 SPEAR T-cell. The ability to administer our SPEAR T-cells to patients in accordance with set protocols for the clinical trials and the results obtained depends on patient participation for the duration of the clinical trial, which many of these patients are unable to do because of their late-stage cancer and limited life expectancy.
Although the initial results in our clinical trials to date may suggest a promising tolerability profile, these results may not be indicative of results obtained in later and larger clinical trials. Long-term follow-up of patients from earlier trials may also result in detection of additional side effects or identification of other safety issues. There is no guarantee of success in any clinical trial and there is a very high attrition rate for pharmaceutical or biological compounds entering clinical trials. Any side effects or negative safety issues identified at any stage of clinical development will require additional investigation and assessment which can result in additional costs and resource requirements that could delay or potentially terminate our clinical trials.
We may face difficulty in enrolling patients in our clinical trials.
We may find it difficult to enroll patients in our clinical trials. For example, in our Phase 1/2 melanoma trial with our NY-ESO SPEAR T-cell, there was a delay in enrollment as a result of competition from other emerging therapies. Identifying and qualifying patients, including testing of patients for appropriate target peptides and HLA type, to participate in clinical trials of our SPEAR T-cells are critical to our success. The patient population in which any required peptide antigen is presented may be lower than expected which will increase the timescales required to find and recruit patients into the applicable clinical trial. For example, fewer patients expressing the required peptide antigens in the Company’s NSCLC clinical trials with its NY-ESO SPEAR T-cell and MAGE-A10 SPEAR T-cell have been seen than anticipated. The timing of our clinical trials depends on the speed at which we can recruit patients to participate in testing our SPEAR T-cells. If patients are unwilling to participate in our trials because of negative publicity from adverse events or for other reasons, including competitive clinical trials for similar patient populations, negative results seen in competitive third party clinical trials utilizing similar cell therapy products, the timeline for recruiting patients, conducting trials and obtaining regulatory approval of potential products may be delayed or prevented. These delays could result in increased costs, delays in advancing our product development, delays in testing the effectiveness of our technology or termination of the clinical trials altogether. We may not be able to identify, recruit and enroll a sufficient number of patients, or those with required or desired characteristics to achieve sufficient diversity in a given trial in order to complete our clinical trials in a timely manner. Patient enrollment is affected by factors including:
· eligibility criteria for the trial in question, in particular, presenting the correct HLA type and expression levels of the target antigen;
· ability to detect required expression levels of target antigens in any patient population;
· ability to detect required target antigens in any patient population and to set detection levels at an appropriate level to facilitate patient recruitment;
· severity of the disease under investigation;
· design of the trial protocol;
· size of the patient population;
· perceived risks and benefits of the SPEAR T-cell under trial;
· novelty of the SPEAR T-cell and acceptance by oncologists;
· proximity and availability of clinical trial sites for prospective patients;
40
Table of Contents
· availability of competing therapies and clinical trials;
· efforts to facilitate timely enrollment in clinical trials;
· patient referral practices of physicians;
· changes in the underlying standard of care applicable or treatments available for the relevant indication for which a patient is being treated; and
· ability to monitor patients adequately during and after treatment.
If we have difficulty enrolling a sufficient number of patients to conduct our clinical trials as planned, we may need to delay, limit or terminate ongoing or planned clinical trials, any of which would have an adverse effect on our business.
Our SPEAR T-cells for which we intend to seek approval as biologic products may face competition sooner than anticipated.
The enactment of the Biologics Price Competition and Innovation Act of 2009, or BPCIA, created an abbreviated pathway for the approval of biosimilar and interchangeable biological products. The abbreviated regulatory pathway establishes legal authority for the FDA to review and approve biosimilar biologics, including the possible designation of a biosimilar as “interchangeable” based on its similarity to an existing reference product. Under the BPCIA, an application for a biosimilar product cannot be approved by the FDA until 12 years after the original branded product is approved under a BLA. On March 6, 2015, the FDA approved the first biosimilar product under the BPCIA. However, the law is complex and is still being interpreted and implemented by the FDA and as a result, its ultimate impact, implementation and meaning are subject to uncertainty. While it is uncertain when such processes intended to implement BPCIA may be fully adopted by the FDA, any such processes could have a material adverse effect on the future commercial prospects for our biological products.
We believe that if our NY-ESO SPEAR T-cell is approved as a biological product under a BLA it should qualify for the 12-year period of exclusivity. However, there is a risk that the FDA will not consider our NY-ESO SPEAR T-cell or any additional SPEAR T-cells to be reference products for competing products, potentially creating the opportunity for generic competition sooner than anticipated. Additionally, this period of regulatory exclusivity does not apply to companies pursuing regulatory approval via their own traditional BLA, rather than via the abbreviated pathway. Moreover, the extent to which a biosimilar, once approved, will be substituted for any one of our reference products in a way that is similar to traditional generic substitution for non-biological products is not yet clear, and will depend on a number of marketplace and regulatory factors that are still developing.
Foreign countries also have abbreviated regulatory pathways for biosimilars and hence even where the FDA does not approve a biosimilar biologic, a biosimilar could be approved using an abbreviated regulatory pathway in other markets where our SPEAR T-cells are approved and marketed.
Risks Related to Government Regulation
The FDA regulatory approval process is lengthy and time- consuming, and we may experience significant delays in the clinical development and regulatory approval of our SPEAR T-cells.
We have not previously submitted a BLA to the FDA, or similar approval submissions to comparable foreign authorities. A BLA must include extensive preclinical and clinical data and supporting information to establish the SPEAR T-cell’s safety and effectiveness for each desired indication. The BLA must also include significant information regarding the chemistry, manufacturing and controls for the product. We expect the novel nature of our SPEAR T-cells to create additional challenges in obtaining regulatory approval, if at all. For example, the FDA has limited experience with commercial development of T-cell therapies for cancer. Accordingly, the regulatory approval pathway for our SPEAR T-cells may be uncertain, complex, expensive and lengthy, and approval may not be obtained. In relation to our NY-ESO SPEAR T-cell in synovial sarcoma, the FDA has requested certain additional information be made available as part of the Company’s application to conduct a pivotal study in synovial sarcoma, including a requirement to assess comparability between the manufacturing process used for the initial synovial sarcoma trials and the commercial-ready manufacturing process intended to be used in pivotal trials. The FDA also recommended that the Company file a SPA in relation to the design of the pivotal study. Such requirements and requests for additional information can delay the start of the pivotal trial and there is no guarantee that the FDA will not continue to require further or additional information ahead of approving any pivotal trial.
41
Table of Contents
We could also encounter delays if physicians encounter unresolved ethical issues associated with enrolling patients in clinical trials of our SPEAR T-cells in lieu of prescribing existing treatments that have established safety and efficacy profiles. Further, a clinical trial may be suspended or terminated by us, the sponsor of an investigator-initiated trial, IRBs for the institutions in which such trials are being conducted, the Data Monitoring Committee for such trial, or by the FDA or other regulatory authorities due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols, inspection of the clinical trial operations or trial site by the FDA or other regulatory authorities resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from using a SPEAR T-cell, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial. If we experience termination of, or delays in the completion of, any clinical trial of our SPEAR T-cells, the commercial prospects for our SPEAR T-cells will be harmed, and our ability to generate product revenue will be delayed. In addition, any delays in completing our clinical trials will increase our costs, slow our product development and approval process and jeopardize our ability to commence product sales and generate revenue.
Many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials may ultimately lead to the denial of regulatory approval of our SPEAR T-cells.
The FDA regulatory process can be difficult to predict, in particular whether for example accelerated approval processes are available or further unanticipated clinical trials are required will depend on the data obtained in our ongoing clinical trials.
The regulatory approval process and the amount of time it takes us to obtain regulatory approvals for our SPEAR T-cells will depend on the data that are obtained in our ongoing clinical trials and in one or more future registration or pivotal clinical trials. We may attempt to seek approval on a per indication basis for our SPEAR T-cells on the basis of a single pivotal trial. While the FDA requires in most cases two adequate and well-controlled pivotal clinical trials to demonstrate the efficacy of a product candidate, a single pivotal trial with other confirmatory evidence may be sufficient in rare instances where the trial is a large multicenter trial demonstrating internal consistency and a statistically very persuasive finding of a clinically meaningful effect on mortality, irreversible morbidity or prevention of a disease with a potentially serious outcome and confirmation of the result in a second trial would be practically or ethically impossible. Depending on the data we obtain, the FDA or other regulatory authorities may require additional clinical trials to be carried out or further patients to be treated prior to the granting of any regulatory approval for marketing of our SPEAR T-cells. It is difficult for us to predict with such a novel technology exactly what will be required by the regulatory authorities in order to take our SPEAR T-cells to market or the timeframes under which the relevant regulatory approvals can be obtained.
We have obtained breakthrough therapy status for our NY-ESO SPEAR T-cell for the treatment of certain patients with inoperable or metastatic synovial sarcoma who have received prior chemotherapy. Depending on the data that is obtained by us in our current and future clinical trials in other indications for our NY-ESO SPEAR T-cell or for our other SPEAR T-cells, we may seek breakthrough therapy or fast track designation or accelerated approval from the FDA for our SPEAR T-cells and equivalent accelerated approval procedures in other countries. However, given the novel nature of our SPEAR T-cells, it is difficult for us to predict or guarantee whether the FDA or other regulatory authorities will approve such requests or what further clinical or other data may be required to support an application for such accelerated approval procedures.
The process of obtaining marketing approvals, both in the United States and abroad, is expensive, may take many years if additional clinical trials are required, if approval is obtained at all, and can vary substantially based upon a variety of factors, including the type, complexity and novelty of the SPEAR T-cells involved. Changes in marketing approval policies during the development period, changes in or the enactment of additional statutes or regulations, or changes in regulatory review for each submitted product application, may cause delays in the approval or rejection of an application. The FDA and foreign regulatory authorities also have substantial discretion in the drug and biologics approval process. The number and types of preclinical programs and clinical trials that will be required for regulatory approval varies depending on the SPEAR T-cell, the disease or condition that the SPEAR T-cell is designed to address, and the regulations applicable to any particular SPEAR T-cell. Approval policies, regulations or the type and amount of clinical data necessary to gain approval may change during the course of a SPEAR T-cell’s clinical development and may vary among jurisdictions, and there may be varying interpretations of data obtained from preclinical programs or clinical trials, either of which may cause delays or limitations in the approval or the decision not to approve an application. In addition, approval of our SPEAR T-cells could be delayed or refused for many reasons, including the following:
· the FDA or comparable foreign regulatory authorities may disagree with the design or implementation of our clinical trials;
· we may be unable to demonstrate to the satisfaction of the FDA or comparable foreign regulatory authorities that our SPEAR T-cells are safe and effective for any of their proposed indications;
· the results of clinical trials may not meet the level of statistical significance required by the FDA or comparable foreign regulatory authorities for approval;
42
Table of Contents
· we may be unable to demonstrate that our SPEAR T-cells’ clinical and other benefits outweigh their safety risks;
· the FDA or comparable foreign regulatory authorities may disagree with our interpretation of data from preclinical programs or clinical trials;
· the data collected from clinical trials of our SPEAR T-cells may not be sufficient to the satisfaction of the FDA or comparable foreign regulatory authorities to support the submission of a BLA or other comparable submission in foreign jurisdictions or to obtain regulatory approval in the United States or elsewhere;
· our manufacturing processes or facilities or those of the third-party manufacturers with which we may not be adequate to support approval of our SPEAR T-cells; and
· the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval.
It is possible that none of our SPEAR T-cells will ever obtain the appropriate regulatory approvals necessary to commercialize the TCR therapeutics. Any delay in obtaining, or failure to obtain, required approvals would materially adversely affect our ability to generate revenue from the particular SPEAR T-cell, which would result in significant harm to our business.
Obtaining and maintaining regulatory approval of our SPEAR T-cells in one jurisdiction does not mean that we will be successful in obtaining regulatory approval of our SPEAR T-cells in other jurisdictions.
Obtaining and maintaining regulatory approval of our SPEAR T-cells in one jurisdiction does not guarantee that we will be able to obtain or maintain regulatory approval in any other jurisdiction, while a failure or delay in obtaining regulatory approval in one jurisdiction may have a negative effect on the regulatory approval process in others. For example, even if the FDA grants marketing approval of a SPEAR T-cell, comparable regulatory authorities in foreign jurisdictions must also approve the manufacturing, marketing and promotion of the SPEAR T-cell in those countries. Approval procedures vary among jurisdictions and can involve requirements and administrative review periods different from, and greater than, those in the United States, including additional preclinical programs or clinical trials as clinical trials conducted in one jurisdiction may not be accepted by regulatory authorities in other jurisdictions. In many jurisdictions outside the United States, a SPEAR T-cell must be approved for reimbursement before it can be approved for sale in that jurisdiction. In some cases, the price that we intend to charge for our SPEAR T-cells is also subject to approval.
We may also submit marketing applications in other countries. Regulatory authorities in jurisdictions outside of the United States have requirements for approval of SPEAR T-cells with which we must comply prior to marketing in those jurisdictions. Obtaining foreign regulatory approvals and compliance with foreign regulatory requirements could result in significant delays, difficulties and costs for us and could delay or prevent the introduction of our SPEAR T-cells in certain countries. If we fail to comply with the regulatory requirements in international markets and/or receive applicable marketing approvals, our target market will be reduced and our ability to realize the full market potential of our SPEAR T-cells will be harmed.
We plan to seek breakthrough therapy or fast track designations and may pursue accelerated approval for some or all of our current SPEAR T-cells, but we may be unable to obtain such designations or, in the case of NY-ESO, maintain its breakthrough therapy designation or, obtain or maintain the benefits associated with such designations.
We have obtained breakthrough therapy status for our NY-ESO SPEAR T-cell for the treatment of certain patients with inoperable or metastatic synovial sarcoma who have received prior chemotherapy. We may seek breakthrough therapy or fast track designations for our other SPEAR T-cells in the United States or equivalent regulations elsewhere in the world or in other indications for our NY-ESO SPEAR T-cell.
In 2012, the FDA established a breakthrough therapy designation which is intended to expedite the development and review of products that treat serious or life-threatening diseases when “preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development.” The designation of a SPEAR T-cell as a breakthrough therapy provides potential benefits that include more frequent meetings with the FDA to discuss the development plan for the SPEAR T-cell and ensure collection of appropriate data needed to support approval; more frequent written correspondence from the FDA about things such as the design of the proposed clinical trials and use of biomarkers; intensive guidance on an efficient drug development program, beginning as early as Phase 1; organizational commitment involving senior managers; and eligibility for rolling review and priority review.
Breakthrough therapy designation does not change the standards for product approval. There can be no assurance that we will receive breakthrough therapy designation for any SPEAR T-cell or any particular indication. Additionally, other treatments from competing companies may obtain the designations and impact our ability to develop and commercialize our SPEAR T-cells, which may adversely impact our business, financial condition or results of operation.
43
Table of Contents
We may also seek fast track designation. If a drug or biologic candidate is intended for the treatment of a serious or life-threatening condition or disease and the drug demonstrates the potential to address unmet medical needs for the condition, the sponsor may apply for fast track designation. Under the fast track program, the sponsor of a new drug or biologic candidate may request that the FDA designate the candidate for a specific indication as a fast track drug or biologic concurrent with, or after, the submission of the IND for the candidate. The FDA must determine if the drug or biologic candidate qualifies for fast track designation within 60 days of receipt of the sponsor’s request. Even if we do apply for and receive fast track designation, we may not experience a faster development, review or approval process compared to conventional FDA procedures. The FDA may withdraw fast track designation if it believes that the designation is no longer supported by data from our clinical development program.
We may also seek accelerated approval under the FDA’s fast track and accelerated approval programs, the FDA may approve a drug or biologic for a serious or life-threatening illness that provides meaningful therapeutic benefit to patients over existing treatments based upon a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. For drugs granted accelerated approval, post-marketing confirmatory trials have been required to describe the anticipated effect on irreversible morbidity or mortality or other clinical benefit. These confirmatory trials must be completed with due diligence. Moreover, the FDA may withdraw approval of our SPEAR T-cell or indication approved under the accelerated approval pathway if, for example:
· the trial or trials required to verify the predicted clinical benefit of our SPEAR T-cell fail to verify such benefit or do not demonstrate sufficient clinical benefit to justify the risks associated with the drug;
· other evidence demonstrates that our SPEAR T-cell is not shown to be safe or effective under the conditions of use;
· we fail to conduct any required post approval trial of our SPEAR T-cell with due diligence; or
· we disseminate false or misleading promotional materials relating to the relevant SPEAR T-cell.
Even if we receive regulatory approval of our SPEAR T-cells, we will be subject to ongoing regulatory obligations and continued regulatory review, which may result in significant additional expense as well as significant penalties if we fail to comply with regulatory requirements or experience unanticipated problems with our SPEAR T-cells.
Any regulatory approvals that we receive for our SPEAR T-cells will require surveillance to monitor the safety and efficacy of the SPEAR T-cell. The FDA may also require a risk evaluation and mitigation strategy in order to approve our SPEAR T-cells, which could entail requirements for a medication guide, physician communication plans or additional elements to ensure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. In addition, if the FDA or a comparable foreign regulatory authority approves our SPEAR T-cells, the manufacturing processes, labeling, packaging, distribution, adverse event reporting, storage, advertising, promotion, import, export and recordkeeping for our SPEAR T-cells will be subject to extensive and ongoing regulatory requirements. These requirements include submissions of safety and other post-marketing information and reports, registration and listing, as well as continued compliance with cGMPs and cGCPs for any clinical trials that we conduct post-approval. We and our contract manufacturers will be subject to periodic unannounced inspections by the FDA to monitor and ensure compliance with cGMPs. We must also comply with requirements concerning advertising and promotion for any SPEAR T-cells for which we obtain marketing approval. Promotional communications with respect to prescription drugs, including biologics, are subject to a variety of legal and regulatory restrictions and must be consistent with the information in the product’s approved labeling. Thus, we will not be able to promote any SPEAR T-cells we develop for indications or uses for which they are not approved. Later discovery of previously unknown problems with our SPEAR T-cells, including adverse events of unanticipated severity or frequency, or with our third-party manufacturers or manufacturing processes, or failure to comply with regulatory requirements, may result in, among other things:
· restrictions on our ability to conduct clinical trials, including full or partial clinical holds on ongoing or planned trials;
· restrictions on such products’ manufacturing processes;
· restrictions on the marketing of a product;
· restrictions on product distribution;
· requirements to conduct post-marketing clinical trials;
· untitled or warning letters;
44
Table of Contents
· withdrawal of the products from the market;
· refusal to approve pending applications or supplements to approved applications that we submit;
· recall of products;
· fines, restitution or disgorgement of profits or revenue;
· suspension or withdrawal of regulatory approvals;
· refusal to permit the import or export of our products;
· product seizure;
· injunctions;
· imposition of civil penalties; or
· criminal prosecution.
The FDA’s and other regulatory authorities’ policies may change and additional government regulations may be enacted that could prevent, limit or delay regulatory approval of our SPEAR T-cells. We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action, either in the United States or abroad. If we are slow or unable to adapt to changes in existing requirements or the adoption of new requirements or policies, or if we are not able to maintain regulatory compliance, we may lose any marketing approval that we may have obtained and we may not achieve or sustain profitability.
In addition, if following a pivotal clinical trial we were able to obtain accelerated approval of our NY-ESO SPEAR T-cell, the FDA will require us to conduct a confirmatory trial or trials to verify the predicted clinical benefit and additional safety studies. The results from the confirmatory trial or trials may not support the clinical benefit, which would result in the approval being withdrawn.
We may seek a conditional marketing authorization in Europe for some or all of our current SPEAR T-cells, but we may not be able to obtain or maintain such authorization.
As part of its marketing authorization process, the EMA may grant marketing authorizations for certain categories of medicinal products on the basis of less complete data than is normally required, when doing so may meet unmet medical needs of patients and serve the interest of public health. In such cases, it is possible for the Committee for Medicinal Products for Human Use, or CHMP, to recommend the granting of a marketing authorization, subject to certain specific obligations to be reviewed annually, which is referred to as a conditional marketing authorization. This may apply to medicinal products for human use that fall under the jurisdiction of the EMA, including those that aim at the treatment, the prevention, or the medical diagnosis of seriously debilitating diseases or life-threatening diseases and those designated as orphan medicinal products.
A conditional marketing authorization may be granted when the CHMP finds that, although comprehensive clinical data referring to the safety and efficacy of the medicinal product have not been supplied, all the following requirements are met:
· the risk-benefit balance of the medicinal product is positive;
· it is likely that the applicant will be in a position to provide the comprehensive clinical data;
· unmet medical needs will be fulfilled; and
· the benefit to public health of the immediate availability on the market of the medicinal product concerned outweighs the risk inherent in the fact that additional data is still required.
The granting of a conditional marketing authorization is restricted to situations in which only the clinical part of the application is not yet fully complete. Incomplete preclinical or quality data may only be accepted if duly justified and only in the case of a product intended to be used in emergency situations in response to public-health threats. Conditional marketing authorizations are valid for one year, on a renewable basis. The holder will be required to complete ongoing trials or to conduct new trials with a view to confirming that the benefit-risk balance is positive. In addition, specific obligations may be imposed in relation to the collection of pharmacovigilance data.
45
Table of Contents
Granting a conditional marketing authorization allows medicines to reach patients with unmet medical needs earlier than might otherwise be the case and will ensure that additional data on a product are generated, submitted, assessed and acted upon. Although we may seek a conditional marketing authorization for one or more of our SPEAR T-cells by the EMA, the EMA or CHMP may ultimately not agree that the requirements for such conditional marketing authorization have been satisfied and hence delay the commercialization of our SPEAR T-cells.
We may not be able to obtain or maintain orphan drug exclusivity for our SPEAR T-cells.
Regulatory authorities in some jurisdictions, including the United States and Europe, may designate drugs or biologics for relatively small patient populations as orphan drugs. Under the Orphan Drug Act, the FDA may designate a product as an orphan drug if it is a drug or biologic intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals in the United States.
Generally, if a product with an orphan drug designation subsequently receives the first marketing approval for the indication for which it has such designation, the product is entitled to a period of marketing exclusivity, which precludes the EMA or the FDA from approving another marketing application for the same drug for that time period. The applicable period is seven years in the United States and 10 years in Europe. The European exclusivity period can be reduced to six years if a drug no longer meets the criteria for orphan drug designation or if the drug is sufficiently profitable so that market exclusivity is no longer justified. Orphan drug exclusivity may be lost if the FDA or EMA determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the drug to meet the needs of patients with the rare disease or condition.
Orphan drug designation for our NY-ESO SPEAR T-cell for the treatment of soft tissue sarcoma was granted by the FDA in March 2016. Some of our other SPEAR T-cells or the indications which our SPEAR T-cells are used to treat may be eligible for orphan drug designation. In the United States, under the Orphan Drug Act, the FDA may grant orphan designation to a drug intended to treat a rare disease or condition. Such diseases and conditions are those that affect fewer than 200,000 individuals in the United States or, if they affect more than 200,000 individuals in the United States, there is no reasonable expectation that the cost of developing and making a drug product available in the United States for these types of diseases or conditions will be recovered from sales of the product. If the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by that agency. Orphan drug designation does not convey any advantage in or shorten the duration of the regulatory review and approval process, but it can lead to financial incentives, such as opportunities for grant funding toward clinical trial costs, tax advantages in-lieu of R&D tax credits and user-fee waivers. If a product that has orphan drug designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan drug marketing exclusivity for a period of seven years. Orphan drug marketing exclusivity generally prevents the FDA from approving another application, including a full BLA, to market the same drug for the same indication for seven years, except in limited circumstances, including if the FDA concludes that the later drug is clinically superior to the approved drug.
Orphan drug designation for the company’s NY-ESO SPEAR T-cell for the treatment of soft tissue sarcoma, a solid tumor cancer has also been granted by the European Union. Orphan drug designation provides certain regulatory and financial incentives for companies to develop and market therapies that treat a life-threatening or chronically debilitating condition affecting no more than five in 10,000 persons in the European Union, and where no satisfactory treatment is available. The designation provides incentives for companies seeking protocol assistance and scientific advice from the EMA during the product development phase and a 10-year period of marketing exclusivity in the European Union following product approval.
A drug is clinically superior if it is safer, more effective or makes a major contribution to patient care. Orphan drug marketing exclusivity rights in the United States may be lost if the FDA later determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the drug to meet the needs of patients with the rare disease or condition. There can be no assurance that any SPEAR T-cell will be eligible for orphan drug designation in the United States or in other jurisdictions or that it will obtain orphan drug marketing exclusivity upon approval or that we will not lose orphan drug designation for our NY-ESO SPEAR T-cell. Inability to obtain orphan drug designation for a specific SPEAR T-cell or loss of such designation for our NY-ESO SPEAR T-cell in the future would prevent us from taking advantage of the financial benefits associated with orphan drug designation and would preclude us from obtaining marketing exclusivity upon approval, if any. Even if we obtain orphan drug exclusivity for a product, that exclusivity may not effectively protect the product from competition because different drugs can be approved for the same condition. The extent of market exclusivity which is obtained may also be affected if the indication for any relevant registration or pivotal trial is narrower than the orphan designation granted. Even after an orphan drug is approved, the FDA can subsequently approve another drug for the same condition if the FDA concludes that the later drug is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care.
46
Table of Contents
Any failure by us to comply with existing regulations could harm our reputation and operating results.
The production of our SPEAR T-cells is highly regulated and subject to constant inspection. The regulatory environment may also change from time to time. Any failure to comply with regulatory requirements, whether in the United States or in other countries in which our SPEAR T-cells are supplied, may result in investigation by regulatory authorities, suspension of regulatory authorizations and, as a result, suspension of clinical programs or ability to supply any of our SPEAR T-cells and potentially significant fines or other penalties being imposed in relation to any breach. Any failure may also harm our reputation and impact our ability going forward to obtain regulatory approvals for other SPEAR T-cells or require us to undertake additional organizational changes to minimize the risk of further breach.
Our research and development activities utilize hazardous, radioactive and biological materials. Should such materials cause injury or be used other than in accordance with applicable laws and regulations, we may be liable for damages.
We use, hazardous and biological reagents and materials in our research and development at our U.K. site. We also use radioactive reagents and materials in our research and development in the United Kingdom. We have obtained the appropriate certification or ensured that such certification has been obtained as required for the use of these reagents but our use is subject to compliance with applicable laws and there is a risk that should any third party or employee suffer injury or damage from radioactive, hazardous or biological reagents that we may incur liability or obligations to compensate such third parties or employees. We have employer’s liability insurance capped at £10.0 million per occurrence and public liability insurance capped at £3.0 million per occurrence; however, these amounts may be insufficient to compensate us if these events actually occur in the future.
We are subject to the U.K. Bribery Act, the U.S. Foreign Corrupt Practices Act and other anti-corruption laws, as well as export control laws, customs laws, sanctions laws and other laws governing our operations. If we fail to comply with these laws, we could be subject to civil or criminal penalties, other remedial measures, and legal expenses, which could adversely affect our business, results of operations and financial condition.
Our operations are subject to anti-corruption laws, including the U.K. Bribery Act 2010, or Bribery Act, the U.S. Foreign Corrupt Practices Act, or FCPA, and other anti-corruption laws that apply in countries where we do business. The Bribery Act, the FCPA and these other laws generally prohibit us and our employees and intermediaries from bribing, being bribed or making other prohibited payments to government officials or other persons to obtain or retain business or gain some other business advantage. Under the Bribery Act, we may also be liable for failing to prevent a person associated with us from committing a bribery offense. We and our commercial partners may operate in a number of jurisdictions that pose a high risk of potential Bribery Act or FCPA violations, and we participate in collaborations and relationships with third parties whose actions, if non-compliant, could potentially subject us to liability under the Bribery Act, FCPA or local anti-corruption laws. In addition, we cannot predict the nature, scope or effect of future regulatory requirements to which our international operations might be subject or the manner in which existing laws might be administered or interpreted.
We are also subject to other laws and regulations governing our international operations, including regulations administered by the governments of the United Kingdom and the United States, and authorities in the European Union, including applicable export control regulations, economic sanctions on countries and persons, anti-money laundering laws, customs requirements and currency exchange regulations, collectively referred to as the Trade Control laws.
However, there is no assurance that we will be completely effective in ensuring our compliance with all applicable anti-corruption laws, including the Bribery Act, the FCPA or other legal requirements, including Trade Control laws. If we are not in compliance with the Bribery Act, the FCPA and other anti-corruption laws or Trade Control laws, we may be subject to criminal and civil penalties, disgorgement and other sanctions and remedial measures, and legal expenses, which could have an adverse impact on our business, financial condition, results of operations and liquidity. Likewise, any investigation of any potential violations of the Bribery Act, the FCPA, other anti-corruption laws or Trade Control laws by U.K., U.S. or other authorities could also have an adverse impact on our reputation, our business, results of operations and financial condition.
If we are found in violation of federal or state “fraud and abuse” or other health care laws, we may be required to pay a penalty and/or be suspended from participation in federal or state health care programs, which may adversely affect our business, financial condition and results of operations.
If we obtain marketing approval for our products in the United States, if at all, we will be subject to various federal and state health care “fraud and abuse” and other health care laws. Healthcare providers, physicians and third-party payors play a primary role in the recommendation and use of pharmaceutical products that are granted marketing approval. Accordingly, arrangements with third-party payors, existing or potential customers and referral sources are subject to broadly applicable fraud and abuse and other healthcare laws and regulations, and these laws and regulations may constrain the business or financial arrangements and relationships through which manufacturers market, sell and distribute the products for which they obtain marketing approval.
47
Table of Contents
Such restrictions under applicable federal and state healthcare laws and regulations include the following:
· the federal Anti-Kickback Statute, which prohibits, among other things, persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, in cash or kind, in exchange for, or to induce, either the referral of an individual for, or the purchase, order or recommendation of, any good or service for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs. This statute has been interpreted to apply to arrangements between pharmaceutical manufacturers, on the one hand, and prescribers, purchasers and formulary managers on the other. Cases have been brought under false claims laws alleging that off-label promotion of pharmaceutical products or the provision of kickbacks has resulted in the submission of false claims to governmental health care programs. The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, collectively, the Healthcare Reform Act, amended the intent requirement of the federal Anti-Kickback Statute. A person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. Under federal government regulations, some arrangements, known as safe harbors, are deemed not to violate the federal Anti-Kickback Statute and analogous state law requirements;
· the federal False Claims Act, or FCA, which prohibits, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid or other third-party payors that are false or fraudulent. Federal Anti-Kickback Statute violations and certain marketing practices, including off-label promotion, also may implicate the FCA. In addition, private individuals have the ability to bring actions on behalf of the government under the FCA and under the false claims laws of several states;
· federal criminal laws that prohibit executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters;
· the federal Physician Payment Sunshine Act, which requires certain manufacturers of drugs, devices, biologics and medical supplies to report annually to the Centers for Medicare & Medicaid Services, or CMS, information related to payments and other transfers of value to physicians, other healthcare providers and teaching hospitals, and ownership and investment interests held by physicians and other healthcare providers and their immediate family members. The CMS publishes the reported data in a searchable form on an annual basis;
· The Health Insurance Portability and Accountability Act of 1996 (HIPAA) imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters;
· HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, which governs the conduct of certain electronic healthcare transactions and protects the security and privacy of protected health information; and
· state and foreign law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to: items or services reimbursed by any third-party payor, including commercial insurers; state laws that require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance issued by the federal government or otherwise restrict payments that may be made to healthcare providers and other potential referral sources; state laws that require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures; and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts. California and a few other states have passed laws that require pharmaceutical companies to comply with the April 2003 Office of Inspector General Compliance Program Guidance for Pharmaceutical Manufacturers and/or the Pharmaceutical Research and Manufacturers of America Code on Interactions with Healthcare Professionals. In addition, several states impose other marketing restrictions or require pharmaceutical companies to make marketing or price disclosures to the state. There are ambiguities as to what is required to comply with these state requirements and if we fail to comply with an applicable state law requirement we could be subject to penalties.
48
Table of Contents
Neither the government nor the courts have provided definitive guidance on the application of fraud and abuse laws to our business. Law enforcement authorities are increasingly focused on enforcing these laws. Although we seek to structure our business arrangements in compliance with all applicable requirements, these laws are broadly written, and it is often difficult to determine precisely how the law will be applied in specific circumstances. Accordingly, it is possible that, once we begin marketing our product(s) some of our practices may be challenged under these laws. While we intend to structure our business arrangements to comply with these laws, it is possible that the government could allege violations of, or convict us of violating, these laws. Violation of any of the laws described above or any other governmental laws and regulations may result in penalties, including civil and criminal penalties, damages, fines, the curtailment or restructuring of operations, the exclusion from participation in federal and state healthcare programs and imprisonment. Furthermore, efforts to ensure that business activities and business arrangements comply with applicable healthcare laws and regulations can be costly for manufacturers of branded prescription products. Additionally, if we are found in violation of one or more of these laws our business, results of operations and financial condition may be adversely affected.
Our current cash projections include reliance on the ability to obtain certain tax credits and the operation of certain tax regimes with in the United Kingdom. Should these cease to be available, this could impact our ongoing requirement for investment and the timeframes within which additional investment is required.
As a company that carries out extensive research and development activities, we benefit from the U.K. research and development tax credit regime for small and medium sized companies, whereby our principal research subsidiary company, Adaptimmune Limited, is able to surrender the trading losses that arise from its research and development activities for a payable tax credit of up to approximately 33.4% of eligible research and development expenditures. Qualifying expenditures largely comprise employment costs for research staff, consumables and certain internal overhead costs incurred as part of research projects. Subcontracted research expenditures are eligible for a cash rebate of up to approximately 21.7%. The majority of our pipeline research, clinical trials management and manufacturing development activities, all of which are being carried out by Adaptimmune Limited, are eligible for inclusion within these tax credit cash rebate claims.
We may not be able to continue to claim research and development tax credits (R&D tax credits) in the future as we increase our personnel and expand our business because we may no longer qualify as an SME (small or medium-sized enterprise). In order to qualify as an SME for R&D tax credits, we must continue to be a company with fewer than 500 employees and also have either an annual turnover not exceeding €100 million or a balance sheet not exceeding €86 million.
We may also benefit in the future from the United Kingdom’s “patent box” regime, which would allow certain profits attributable to revenues from patented products to be taxed at a rate that over time will be reduced to 10%. As we have many different patents covering our products, future upfront fees, milestone fees, product revenues, and royalties could be taxed at this favorably low tax rate. When taken in combination with the enhanced relief available on our research and development expenditures, we expect a long-term lower rate of corporation tax to apply to us. If, however, there are unexpected adverse changes to the United Kingdom research and development tax credit regime or the “patent box” regime, or we are unable to qualify for such advantageous tax legislation, our business, results of operations and financial condition may be adversely affected.
Risks Related to the Commercialization of Our SPEAR T-cells
The market opportunities for our SPEAR T-cells may be limited to those patients who have failed prior treatments.
Initial approval of new cancer therapies may be limited to what is referred to as third-line use. Third-line treatment is the third type of treatment following initial, or first-line, treatment and second-line treatment, which is given when first-line treatment does not work or ceases working. However, cancer therapies may be used from the point at which cancer is detected in its early stages (first line) onward. Whenever the first-line therapy fails or the process is unsuccessful, second-line therapy may be administered, such as additional rounds of chemotherapy, radiation and antibody drugs or a combination of these treatments. If second-line therapies fail, patients are generally given the opportunity to receive third-line therapies, which tend to be more novel therapies. Our current clinical trials generally require that patients have received chemotherapy prior to enrollment. Depending upon the outcome of our current trials, we may conduct future clinical trials using our SPEAR T-cells for first-line therapy, but there can be no guarantee that clinical trials will be approved or that if approved such trials will lead to regulatory approval. If our SPEAR T-cells only receive third-line or second-line approval, the patient population to which we can supply our SPEAR T-cells will be significantly reduced, which may limit our commercial opportunities.
Our estimates of the patient population that may be treated by our SPEAR T-cells is based on published information. This information may not be accurate in relation to our SPEAR T-cells and our estimates of potential patient populations could therefore be much higher than those that are actually available or possible for commercialization.
49
Table of Contents
In addition, these estimates are based on assumptions about the number of eligible patients which have the peptide and HLA type targeted by our SPEAR T-cells. Different patient populations will present different peptides according to their specific HLA type. HLA types vary across the patient population and, due to this variability, any therapy will initially only be suitable for treatment of patients expressing the particular HLA type presenting the relevant peptide. Our current SPEAR T-cells have been developed for patients who are HLA A2 which will reduce the size of the patient population that can be treated unless we develop and receive regulatory approval for SPEAR T-cells approved for additional HLA peptides.
We currently have no marketing and sales organization and have no experience in marketing products. If we are unable to establish marketing and sales capabilities or enter into agreements with third parties to market and sell our SPEAR T-cells, we may not be able to generate product revenue.
As an organization, we have never marketed or supplied commercial pharmaceutical or biologic products or therapies. We do not currently have a sales force and will need to grow and develop the sales function and associated support network if we are to supply SPEAR T-cells on a commercial basis. As our SPEAR T-cells proceed through clinical programs, we intend to develop an in-house marketing organization and sales force, which will require significant capital expenditures, management resources, and time. We will have to compete with other pharmaceutical and biotechnology companies to recruit, hire, train, and retain marketing and sales personnel. This process may result in additional delays in bringing our TCR product candidate to market or in certain cases require us to enter into alliances with third parties in order to do so. However, there can be no assurance that we will be able to establish or maintain such collaborative arrangements, or even if we are able to do so, that they will result in effective sales forces. Any revenue we receive will depend upon the efforts of such third parties, which may not be successful. We may have little or no control over the marketing and sales efforts of such third parties, and our revenue from SPEAR T-cell sales may be lower than if we had commercialized our SPEAR T-cells ourselves. We also face significant competition in our search for third parties to assist us with the sales and marketing efforts of our SPEAR T-cells. Such competition may also result in delay or inability to supply SPEAR T-cells to particular countries or territories in the world which in turn will restrict the revenue that can be obtained from any SPEAR T-cell. Any inability on our part to develop in-house sales and commercial distribution capabilities or to establish and maintain relationships with third-party collaborators that can successfully commercialize any SPEAR T-cell in the United States or elsewhere will have a materially adverse effect on our business and results of operations.
If product liability lawsuits are brought against us, we may incur substantial liabilities and may be required to limit commercialization of our SPEAR T-cells.
We face an inherent risk of product liability as a result of the clinical testing of our SPEAR T-cells and will face an even greater risk upon any commercialization. For example, we may be sued if any of our SPEAR T-cells causes or is perceived to cause injury or is found to be otherwise unsuitable during clinical testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability or a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our SPEAR T-cell. Even a successful defense would require significant financial and management resources and, regardless of the merits or eventual outcome, liability claims may result in:
· decreased demand for our SPEAR T-cells;
· injury to our reputation;
· withdrawal of clinical trial participants;
· initiation of investigations by regulators;
· costs to defend the related litigation;
· a diversion of management’s time and our resources;
· substantial monetary awards to trial participants or patients;
· product recalls, withdrawals or labeling, marketing or promotional restrictions;
· loss of revenue;
· exhaustion of any available insurance and our capital resources;
· the inability to commercialize SPEAR T-cells; and
50
Table of Contents
· a decline in our share price.
Our inability to obtain sufficient product liability insurance at an acceptable price to protect against potential product liability claims could also prevent or inhibit the commercialization of our SPEAR T-cells. We currently hold £15.0 million in clinical trial insurance coverage in the aggregate per year, with a per trial limit of £3-4.0 million. We also hold products and services liability insurance capped at £3.0 million in the aggregate and public liability insurance capped at £3.0 million per occurrence. These levels may not be adequate to cover all liabilities that we may incur. We may also need to increase our insurance coverage as we expand the scope of our clinical trials and commercialize any of our product SPEAR T-cells. In addition, insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise.
Even if we obtain regulatory approval of our SPEAR T-cells, they may not gain market acceptance among physicians, patients, hospitals, cancer treatment centers and others in the medical community.
The use of engineered T cells as a potential cancer treatment is a recent development and may not become broadly accepted by physicians, patients, hospitals, cancer treatment centers and others in the medical community. Additional factors will influence whether our SPEAR T-cells are accepted in the market, including:
· the clinical indications for which our SPEAR T-cells are approved;
· physicians, hospitals, cancer treatment centers and patients considering our SPEAR T-cells as a safe and effective treatment;
· the potential and perceived advantages of our SPEAR T-cells over alternative treatments;
· the prevalence and severity of any side effects;
· product labeling or prescribing information requirements of the FDA or other regulatory authorities;
· limitations or warnings contained in the labeling approved by the FDA;
· the timing of market introduction of our SPEAR T-cells as well as competitive products;
· the cost of treatment in relation to alternative treatments;
· the availability of coverage, adequate reimbursement and pricing by third-party payors and government authorities;
· the willingness of patients to pay for our SPEAR T-cell on an out-of-pocket basis in the absence of coverage by third-party payors and government authorities;
· relative convenience and ease of administration as compared to alternative treatments and competitive therapies; and
· the effectiveness of our sales and marketing efforts.
In addition, although we are not utilizing embryonic stem cells or replication competent vectors, adverse publicity due to the ethical and social controversies surrounding the therapeutic use of such technologies, and reported side effects from any clinical trials using these technologies or the failure of such trials to demonstrate that these therapies are safe and effective may limit market acceptance of our SPEAR T-cells. If our SPEAR T-cells are approved but fail to achieve market acceptance among physicians, patients, hospitals, cancer treatment centers or others in the medical community, we will not be able to generate significant revenue.
Even if our SPEAR T-cells achieve market acceptance, we may not be able to maintain that market acceptance over time if new products or technologies are introduced that are more favorably received than our SPEAR T-cells, are more cost effective or render our SPEAR T-cells obsolete.
Coverage and reimbursement may be limited or unavailable in certain market segments for our SPEAR T-cells, which could make it difficult for us to sell our SPEAR T-cells profitably.
Successful sales of our SPEAR T-cells, if approved, depend on the availability of coverage and adequate reimbursement from third-party payors. In addition, because our SPEAR T-cells represent new approaches to the treatment of cancer, we cannot accurately estimate the potential revenue from our SPEAR T-cells.
51
Table of Contents
Patients who are provided medical treatment for their conditions generally rely on third-party payors to reimburse all or part of the costs associated with their treatment. Obtaining coverage and adequate reimbursement from governmental healthcare programs, such as Medicare and Medicaid, and commercial payors is critical to new product acceptance.
Government authorities and third-party payors, such as private health insurers and health maintenance organizations, decide which drugs and treatments they will cover and the amount of reimbursement. Reimbursement by a third-party payor may depend upon a number of factors, including, but not limited to, the third-party payor’s determination that use of a product is:
· a covered benefit under its health plan;
· safe, effective and medically necessary;
· appropriate for the specific patient;
· cost-effective; and
· neither experimental nor investigational.
Obtaining coverage and reimbursement approval of a SPEAR T-cell from a government or other third-party payor is a time-consuming and costly process which could require us to provide to the payor supporting scientific, clinical and cost-effectiveness data for the use of our products. Even if we obtain coverage for a given SPEAR T-cell, the resulting reimbursement payment rates might not be adequate for us to achieve or sustain profitability or may require co-payments that patients find unacceptably high. Patients are unlikely to use our SPEAR T-cells unless coverage is provided and reimbursement is adequate to cover a significant portion of the cost of our SPEAR T-cells.
In the United States, no uniform policy of coverage and reimbursement for products exists among third-party payors. Therefore, coverage and reimbursement for products can differ significantly from payor to payor. As a result, the coverage determination process is often a time-consuming and costly process that will require us to provide scientific and clinical support for the use of our SPEAR T-cells to each payor separately, with no assurance that coverage and adequate reimbursement will be obtained.
We intend to seek approval to market our SPEAR T-cells in both the United States and in selected jurisdictions. If we obtain approval in one or more foreign jurisdictions for our SPEAR T-cells, we will be subject to rules and regulations in those jurisdictions.
In some foreign countries, particularly those in the European Union, the pricing of biologics is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after obtaining marketing approval of a SPEAR T-cell. In addition, market acceptance and sales of our SPEAR T-cells will depend significantly on the availability of coverage and adequate reimbursement from third-party payors for our SPEAR T-cells and may be affected by existing and future health care reform measures.
Third-party payors, whether domestic or foreign, or governmental or commercial, are developing increasingly sophisticated methods of controlling healthcare costs. In both the United States and certain foreign jurisdictions, there have been a number of legislative and regulatory changes to the health care system that could impact our ability to sell our products profitably. In particular, the recently enacted U.S. Healthcare Reform Act and its implementing regulations, among other things, revised the methodology by which rebates owed by manufacturers to the state and federal government for covered outpatient drugs and certain biologics, including our SPEAR T-cells, under the Medicaid Drug Rebate Program are calculated, increased the minimum Medicaid rebates owed by most manufacturers under the Medicaid Drug Rebate Program, extended the Medicaid Drug Rebate program to utilization of prescriptions of individuals enrolled in Medicaid managed care organizations, subjected manufacturers to new annual fees and taxes for certain branded prescription drugs, and provided incentives to programs that increase the federal government’s comparative effectiveness research.
Other legislative changes have been proposed and adopted in the United States since the Healthcare Reform Act was enacted. In August 2011, the Budget Control Act of 2011, among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several government programs.
This includes aggregate reductions of Medicare payments to providers up to two percent per fiscal year, which went into effect on April 1, 2013 and will remain in effect until 2024, unless additional congressional action is taken. In January 2013, President Obama signed into law the American Taxpayer Relief Act of 2012, or the ATRA, which, among other things, reduced Medicare payments to several providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
52
Table of Contents
There have been, and likely will continue to be, legislative and regulatory proposals at the foreign, federal and state levels directed at broadening the availability of healthcare and containing or lowering the cost of healthcare. We cannot predict the initiatives that may be adopted in the future. The continuing efforts of the government, insurance companies, managed care organizations and other payors of healthcare services to contain or reduce costs of healthcare and/or impose price controls may adversely affect:
· the demand for our SPEAR T-cells, if we obtain regulatory approval;
· our ability to set a price that we believe is fair for our SPEAR T-cells;
· our ability to generate revenue and achieve or maintain profitability;
· the level of taxes that we are required to pay; and
· the availability of capital.
Any reduction in reimbursement from Medicare or other government programs may result in a similar reduction in payments from private payors, which may adversely affect our future profitability.
Risks Related to Our Reliance Upon Third Parties
We rely heavily on GSK for our NY-ESO SPEAR T-cell clinical program, which may also affect other SPEAR T-cells.
Our ability to commercialize our NY-ESO SPEAR T-cell and our other SPEAR T-cells depends heavily on the ongoing collaboration with GSK and payments made by GSK to us upon achievement of specified milestones. GSK has the right to nominate three further target programs in addition to the NY-ESO SPEAR T-cell and PRAME SPEAR T-cell programs under the collaboration arrangements. We have no control over whether GSK will elect to progress additional targets under the collaboration arrangements and therefore trigger additional investment from GSK in our SPEAR T-cells. If GSK does not elect to do so, we may require additional capital or investment or need to enter into alternative strategic alliances. In addition, GSK has a right to terminate the collaboration and license agreement or any specific license under the collaboration and license agreement for any reason on provision of sixty days’ notice. Termination may impact not only our requirement for additional investment or capital but also the timeframes within which current clinical programs can be performed and the development of a suitable commercial-scale manufacturing process for any of our SPEAR T-cells. In addition, GSK has an option to obtain an exclusive worldwide license to our NY-ESO SPEAR T-cell program, which is exercisable during specified time periods. If the option is exercised after delivery of required phase I/II data package, GSK will assume full responsibility for our NY-ESO SPEAR T-cell program. There is no guarantee that GSK will exercise the option over the NY-ESO SPEAR T-cell program at all or in the timescales currently anticipated and the timing of option exercise may impact the timing and amount of milestone payments received by the Company.
The current development plans or any future development plan agreed upon between GSK and us may be unsuccessful or fail to result in candidate therapies that are feasible for further development or commercialization. There is therefore no guarantee that any payments due on commercialization of products under the agreement between GSK and us will be due or payable by GSK at any time or on the timeframes currently expected. In addition, milestone payments may not be paid or may be varied where any development plan is amended or where any development plan is terminated prior to completion for lack of feasibility or lack of identification of any suitable candidates that meet the required criteria for progression to the next stage of development.
In addition, the development plans agreed upon with GSK and any future development plans will be subject to change as a result of risks inherent with the development of any pharmaceutical, biological or gene therapy product. Changes may be agreed to expand or change the scope of the collaboration or the responsibilities of the parties under the collaboration. For example, in February 2016 the agreement was expanded to accelerate the development of the NY-ESO SPEAR T-cells towards pivotal trials in synovial sarcoma and provide for additional combination trials. Changes to the development plans or collaboration agreement may impact the timing and extent of milestone payments made by GSK to us, the nature of the relationship with GSK or the scope of the collaboration with GSK.
GSK has the ability to influence or control certain decisions relating to the development of therapies covered by our collaboration and license agreement with GSK. This ability could result in delays to the clinical programs covered by the collaboration or changes to the scope of those clinical programs, including the disease indications relevant to such clinical programs. Under the agreement, we are also prohibited from independently developing or commercializing therapies directed at the targets subject to outstanding options granted to GSK. In addition, GSK may have competing internal or commercial interests including its independent collaboration with Immunocore any of which could impact our collaboration or the ability of GSK to take any clinical programs forward to the next stage following the exercise of their option.
53
Table of Contents
GSK and Novartis have publicly announced that Novartis has opt-in rights over GSK’s current and future oncology research and development pipeline. As part of that announced transaction, GSK has sold the rights to GSK’s marketed oncology portfolio, related R&D activities and the AKT Inhibitors currently in development. GSK has also agreed to grant Novartis preferred partner rights for co-development and commercialization of GSK’s current and future oncology pipeline products for a period of 12.5 years from completion of the applicable transactions between GSK and Novartis. The relevant agreement grants Novartis a right of first negotiation over the co-development or commercialization of any GSK “Relevant Development Product” in a major market. A “Relevant Development Product” as defined in the public announcement is a product in development for the treatment, palliation, diagnosis or prevention of all cancers, including immunology, epigenetics and treatment of solid or hematologic tumors (excluding in all cases, vaccines). The right of first negotiation also lasts for 12.5 years from completion of the applicable transactions between GSK and Novartis and according to the public announcement applies where GSK decides to seek a third party partner for co-development or commercialization of, or to whom to divest rights to, a Relevant Development Product in a global or major market or where GSK proposes to seek a marketing authorization for a Relevant Development Product in a major market.
The existence of these opt-in rights could impact GSK’s decision whether to exercise any option under our collaboration or the ability of GSK to take any clinical programs forward to the next stage, following the exercise of its option.
The relationship with GSK could also result in disputes arising between us and GSK which could result in costly arbitration or litigation and could impact the ongoing clinical programs or progress of such clinical programs. All intellectual property rights arising from the performance of the collaboration and license agreement will be jointly owned apart from intellectual property rights that we solely create. Both GSK and we have freedom to use jointly owned intellectual property rights.
The GSK collaboration programs relate to specific SPEAR T-cells directed to nominated targets. Should any of these programs not be successful or resulting clinical programs show a lack of efficacy or problems with safety, tolerability or durability of response, GSK may decide not to proceed further with such collaboration programs and our ability to obtain other partners for further development of such candidates or of new SPEAR T-cells could be significantly compromised.
We rely heavily on ThermoFisher and the technology that we license from them.
The ability to use the ThermoFisher Dynabeads® CD3/CD28 technology to isolate, activate and expand T cells is important to our ongoing ability to offer SPEAR T-cells. In December 2012, we entered into a series of license and sub-license agreements with Life Technologies Corporation (now part of ThermoFisher). These agreements provide us with a field-based exclusive license under certain intellectual property rights owned or controlled by ThermoFisher in relation to the methods of use of the ThermoFisher Dynabeads® CD3/CD28 technology to isolate, activate and expand T-cells and enable transfection of the T-cells with any TCR genes to manufacture our TCR products and use and sell those TCR products to treat cancer, infectious disease and/or autoimmune disease. We also have a field-based exclusive sub-license under certain other patents which cover the method of use of the Dynabeads® CD3/CD28 and are controlled by ThermoFisher under a head-license from the University of Michigan, the United States Navy and the Dana-Farber Cancer Institute.
In June 2016, we entered into a supply agreement with ThermoFisher for the supply of the Dynabeads® CD3/CD28 technology. The supply agreement runs until December 31, 2025. Under the supply agreement we are required to purchase our requirements for CD3/CD28 magnetic bead product exclusively from ThermoFisher for a period of five years and there are also minimum purchasing obligations. Despite having negotiated this supply agreement there is no certainty that ThermoFisher will be able to continue to supply the Dynabeads® CD3/CD28 technology at the times or at the levels we require or that facilities used by ThermoFisher for the manufacture and supply of the Dynabeads® CD3/CD28 technology will continue to be available to us which could impact the timing of supply of SPEAR T-cells or ability to manufacture SPEAR T-cells.
ThermoFisher has the right to terminate the above described agreements for material breach or insolvency. On termination of the license agreements, the supply agreement will also automatically terminate. If ThermoFisher terminates the exclusive license, sub-license and supply agreements or otherwise refuses or is unable to supply the Dynabeads® product, we will have to seek an alternative source of the beads or develop an alternative process methodology to enable supply of our SPEAR T-cells.
If the supply agreements with ThermoFisher is terminated or ThermoFisher is unable to supply the Dynabeads® CD3/CD28 technology for any reason, an alternative source may be difficult to find or more expensive, which may delay timeframes either for clinical programs or ultimately commercial supply of our SPEAR T-cells. A requirement to identify an alternative source may also require a change in our regulatory application or additional regulatory testing to ensure that any alternative source is comparable and does not present any additional risk which could also result in our program experiencing delays and increased costs.
The sub-license agreement, in addition to having the same relevant exclusivity scope and field-based restrictions and many of the terms being equivalent to those set out in the main license agreement with ThermoFisher, also includes additional requirements that any manufacture of engineered TCR products for sale in the United States must occur in the United States and reserves rights for the United States government to use the technology in accordance with 35 U.S.C. § 200 et seq. and for the University of Michigan and Dana-Farber Cancer Institute to use the technology for non-commercial research purposes.
54
Table of Contents
We rely on third parties to manufacture and supply our SPEAR T-cells, and we may have to rely on third parties to produce and process our SPEAR T-cells, if approved.
We currently rely on outside contract manufacturing organizations (“CMOs”) to manufacture, supply and process our SPEAR T-cells. If one or more of these CMOs become unable or unwilling to continue to manufacture our engineered SPEAR T-cells (including any raw or intermediate material required for the manufacture of our end engineered SPEAR T-cell therapy) in the future, we may be forced to find an alternative third-party manufacturer, which we may not be able to do on commercially reasonable terms, if at all. Failure to identify a suitable alternative manufacturer could impact our business, financial condition or results of operations.
We rely on a limited number of third-party manufacturers for clinical trial product supplies, and if we are unable to develop our own commercial manufacturing facility for any commercial product supplies, we will be exposed to the following risks:
· We may be unable to contract with manufacturers on commercially acceptable terms or at all because the number of potential manufacturers is limited and the FDA, EMA and other comparable foreign regulators must approve any replacement manufacturer, which would require new testing and compliance inspections. In addition, a new manufacturer would have to be educated in, and develop substantially equivalent processes for, production of our SPEAR T-cells after receipt of any applicable regulatory approval.
· We may not be able to obtain lentiviral delivery manufacturing slots with third party contract manufacturers within the timescales we require for supply of lentiviral delivery vector or to obtain agreed dates for such manufacturing slots sufficiently in advance of the requirement for supply.
· Our third-party manufacturers might be unable to timely formulate and manufacture our SPEAR T-cells or produce the quantity and quality required to meet our clinical trial and commercial needs, if any.
· Contract manufacturers may not be able to execute our manufacturing procedures appropriately, or we may be unable to transfer our manufacturing processes to contract manufacturers successfully or without additional time and cost.
· Our future contract manufacturers may not perform as agreed, may be acquired by competitors or may not remain in the contract manufacturing business for the time required to supply our clinical trials or to successfully produce, store and distribute our SPEAR T-cells. In addition contract manufacturers may not manufacture within agreed timescales for manufacture and/or may cancel pre-agreed manufacturing slots, which would result in delays in manufacturing and could require us to find replacement manufacturers which may not be available to us on favorable terms or at all.
· Manufacturers are subject to ongoing periodic unannounced inspection by the FDA, EMA, and other comparable foreign regulators and corresponding state agencies to ensure strict compliance with cGMP and other government regulations and corresponding foreign standards. Although we do not have day-to-day control over third-party manufacturers’ compliance with these regulations and standards, we are responsible for ensuring compliance with such regulations and standards.
· We may not own, or may have to share, the intellectual property rights to any improvements made by our third-party manufacturers in the manufacturing process for our SPEAR T-cells.
· Our third-party manufacturers could breach or terminate their agreement with us
· Our third-party manufacturers may cease to be able to do business with us (whether for insolvency or other reasons, including takeover, merger or acquisition) at a time when we are unable to source such manufacture elsewhere or at our own manufacturing facility.
Certain raw materials or precursor materials used in the manufacture and supply of our SPEAR T-cells may come from sole source or limited source suppliers. For example, there are currently a limited number of third party manufacturers within the United States that can supply us with our lentiviral delivery vector, ThermoFisher is currently the only supplier of the Dynabeads® CD3/CD28 technology and PCT, LLC is currently the only manufacturer of our end SPEAR T-cell therapy. Should such suppliers be unable to supply or manufacture such raw materials or precursor materials either at all or within required timescales we may be unable to supply our SPEAR T-cells or such supply may be significantly delayed. Inability to obtain such raw materials or precursor materials may also necessitate changes in the manufacturing process used for supply of our SPEAR T-cells. Such changes to the manufacturing process may need to be developed internally or by a third party and may also require additional regulatory approvals to be obtained before they can be used for the manufacture and supply of our SPEAR T-cells for clinical trials.
55
Table of Contents
Our contract manufacturers are also subject to the same risks we face in developing our own manufacturing capabilities, as described above. Each of these risks could delay our clinical trials, the approval, if any, of our SPEAR T-cells by the FDA or the commercialization of our SPEAR T-cells or result in higher costs or deprive us of potential product revenue. We have insurance to cover certain costs and expenses related to business interruption, which is capped at £3.0 million in the aggregate.
In addition, we will rely on third parties to perform release tests on our SPEAR T-cells prior to delivery to patients. If these tests are not appropriately performed and test data is not reliable, patients could be put at risk of serious harm.
We have a shared development history with Immunocore, and as a result jointly-own certain intellectual property rights which are required for our ongoing business.
Our TCR technology was originally developed by Avidex, which was subsequently acquired by Medigene in 2006. We were formed as a new, separate company and licensed our TCR technology for T-cell therapy from Medigene in July 2008. Immunocore was subsequently formed as a new separate company and acquired the TCR technology for soluble TCRs from Medigene later in 2008 to develop soluble TCR proteins. Immunocore currently owns approximately 6.35% of the ordinary shares in Adaptimmune. Three of our greater than five percent ordinary shareholders, Nicholas Cross, Ian Laing and George Robinson, are significant shareholders in, and are directors of, Immunocore. Our scientific founder and advisor, Bent Jakobsen, is also an employee of Immunocore.
Both Adaptimmune and Immunocore focus on technologies that are based on TCR therapies. Each company focuses on distinct applications of, and utilizes different, TCRs. Immunocore uses soluble TCRs whereas Adaptimmune uses cellular SPEAR T-cells. Both soluble TCRs and Adaptimmune’s SPEAR T-cells rely on the engineering of TCRs to create affinity-enhanced TCRs. In Adaptimmune’s case, once the engineered affinity-enhanced TCR has been generated, the gene encoding that engineered TCR is transduced into patient T cells. With soluble TCRs, there is no transduction. For soluble TCRs, the engineered affinity-enhanced TCRs are combined with an antibody fragment, anti-CD3, and it is this combined TCR/anti- CD3 candidate that is then used to treat patients directly. The combined candidates are called ImmTACs. As a result, the end therapeutic candidates being developed by each company are different in terms of end structure, affinity, require different manufacturing and administration routes and are likely to have different properties in patients. For example, ImmTACs do not persist beyond a few hours in a patient following administration, whereas Adaptimmune’s TCR therapeutics have been shown to persist in patients for years; ImmTACs are likely to require higher amounts of target peptide to be present and hence Adaptimmune’s TCR therapeutics may address cancer cells with lower levels of antigen; ImmTACs rely on activating the patient’s existing T cells through an anti-CD3-CD3 interaction, whereas Adaptimmune’s SPEAR T-cells activate T cells through direct binding to the target peptide and this results in a different mechanism of action.
Notwithstanding the differences between Immunocore’s and Adaptimmune’s end products, both companies may develop products or therapies that target the same peptide and are directly competitive and/or address the same indications and patient populations. For example, both companies could develop therapeutic candidates to the same peptide target and hence have a product addressing the same patient populations in the same way as any other competing technology. In addition, both Immunocore and Adaptimmune have entered into collaboration agreements with GSK, which could decide over time to devote greater time and resources to Immunocore at the expense of Adaptimmune.
Under the terms of a target collaboration agreement which terminated as of March 1, 2017, we will continue to share a database of identified targets with Immunocore which resulted from the joint target identification efforts under that agreement. The contents of this target database are highly confidential and if disclosed to a third party, either as a result of a breach of the confidentiality terms between us and Immunocore or through a change of control in Immunocore, our business could be adversely impacted.
In addition, many of the patents relating to our underlying core technology in TCR engineering, are co-owned by us and Immunocore pursuant to a separate assignment and license agreement. Under this agreement, each of Immunocore and Adaptimmune utilize the jointly owned patents and know-how, with Adaptimmune focused on the treatment of patients with engineered SPEAR T-cells and Immunocore focused on the treatment of patients with soluble TCRs. Under the agreement, each of Immunocore and Adaptimmune grants the other an exclusive, royalty-free, irrevocable license, with the right to sub-license, to certain jointly owned patents and know-how. However, there is the potential that Immunocore could develop a soluble TCR product targeting the same cancer target that one of our SPEAR T-cells is targeting, and therefore compete directly with us. We also have a transitional services agreement with Immunocore which provides for certain limited ongoing services between the two companies..
56
Table of Contents
We rely on third parties to conduct our clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval of or commercialize our SPEAR T-cells.
We depend upon independent investigators and collaborators, such as universities, medical institutions, CROs and strategic partners to conduct our preclinical programs and sponsored clinical trials under agreements with us. We expect to have to negotiate budgets and contracts with CROs and trial sites (either directly or through a third party consultant), which may result in delays to our development timelines and increased costs. We rely heavily on these third parties over the course of our clinical trials, and we do not have day-to-day control of their activities. Nevertheless, we are responsible for ensuring that each of our trials is conducted in accordance with applicable protocols and legal, regulatory and scientific standards, and our reliance on third parties does not relieve us of our regulatory responsibilities. We and these third parties are required to comply with cGCPs, which are regulations and guidelines enforced by the FDA and comparable foreign regulatory authorities for SPEAR T-cells in clinical development. Regulatory authorities enforce these cGCPs through periodic inspections of trial sponsors, principal investigators and trial sites. If we or any of these third parties fail to comply with applicable cGCP regulations and guidelines, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot provide assurances that, upon inspection, such regulatory authorities will determine that any of our clinical trials comply with the cGCP regulations. In addition, our clinical trials must be conducted with biologic product produced under cGMPs and will require a large number of subjects. Our failure or any failure by these third parties to comply with these regulations or to support BLA for approval of our NY-ESO SPEAR T-cell for the treatment of a sufficient number of patients may require us to repeat clinical trials, which would delay the regulatory approval process. Moreover, our business may be implicated if any of these third parties violates federal or state fraud and abuse or false claims laws and regulations or healthcare privacy and security laws.
Any third parties conducting our clinical trials are not and will not be our employees and, except for remedies available to us under our agreements with such third parties which could be limited, we cannot control whether or not they devote sufficient time and resources to our ongoing clinical trials and preclinical programs. These third parties may also have relationships with other commercial entities, including our competitors, for whom they may also be conducting clinical trials or other drug or biologic development activities, which could affect their performance on our behalf. If these third parties do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols or regulatory requirements or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to complete development of, obtain regulatory approval of, or successfully commercialize our SPEAR T-cells. As a result, our financial results and the commercial prospects for our SPEAR T-cells would be harmed, our costs could increase and our ability to generate revenue could be delayed.
Switching or adding third parties to conduct our clinical trials involves substantial cost and requires extensive management time and focus. In addition, there is a natural transition period when a new third party commences work. As a result, delays may occur, which can materially impact our ability to meet our timelines for bringing our SPEAR T-cells to market, if at all.
In addition to our Company sponsored clinical programs, our NY-ESO TCR therapeutic has also been used in an investigator-initiated clinical program funded by the European Union, referred to as the ATTACK 2 program. The therapy, which was produced under a different manufacturing process than Adaptimmune’s NY-ESO TCR therapy and was administered under a different protocol, was being evaluated for the treatment of patients with advanced gastro-esophageal cancer for the first time. To date, two patients have been treated under this protocol, one of whom passed away 46 days after initial treatment. Said patient experienced enterocolitis and bone marrow failure followed by fatal gangrenous gastrointestinal necrosis and hemorrhage. The investigator determined there was a reasonable possibility that these events were caused by study treatment. Enrollment in the trial was temporarily paused pending investigation of the patient fatality but an independent data monitoring committee has since recommended that recruitment can resume. An amendment to the protocol is currently being considered prior to restarting enrollment in the trial. However, the European Union has terminated funding of the trial due to the delays in trial progression and the Company is in discussions with the sponsor, the Christie NHS Foundation Trust, in relation to continuation of the trial. There is no guarantee we will reach agreement with the Christie NHS Foundation Trust to continue with the esophageal trial at all or on a timely basis.
We rely on third parties to obtain reagents and raw materials.
The manufacture of our SPEAR T-cells requires access to a number of reagents and other raw materials from third parties. Such third parties may refuse to supply such reagents or other raw materials or alternatively refuse to supply on commercially reasonable terms. There may also be capacity issues at such third-party suppliers that impact our ability to increase production of our SPEAR T-cells.
57
Table of Contents
Some of the materials used in the manufacture and processing of our SPEAR T-cells may only be supplied by one or a few vendors, which means that, should those vendors be unable to supply, for whatever reason, our ability to manufacture SPEAR T-cells and progress SPEAR T-cells through clinical trials could be severely impacted and result in additional delays. Such failure to supply could also impact other supply relationships with other third parties and potentially result in additional payments being made or required in relation to such delays. In addition, where any raw material or precursor material (including, for example, lentiviral delivery vector, medium or other essential raw material) is currently supplied by one or a few vendors, replacing such raw material or precursor or finding alternative vendors may not be possible or may significantly impact on the timescales for manufacture and supply of our SPEAR T-cells. Even where alternative materials or precursors or alternative vendors are identified, such alternative materials, precursors or vendors will need to be properly assessed, validated and qualified and additional regulatory approvals may also need to be obtained all of which could result in significant delays to the supply of our SPEAR T-cells or an inability to supply SPEAR T-cells within anticipated timescales, if at all.
Risks Related to Our Intellectual Property
Our SPEAR T-cells could be at risk of biosimilar development.
Expedited routes or abbreviated procedures for obtaining regulatory approval for products aiming to target the same cancer peptide as our SPEAR T-cells may be available to third parties, which we cannot control or prevent. For example, third parties could develop affinity-enhanced TCRs binding to the same targets and regulatory authorities may accept that they are interchangeable with our corresponding SPEAR T-cells and, as a result, grant regulatory approval for such competing products. Entry into the market of such competing products may impact the price of our SPEAR T-cells and the extent of commercialization possible in relation to such SPEAR T-cells.
We may be forced to litigate to enforce or defend our intellectual property rights, and/or the intellectual property rights of our licensors.
We may be forced to litigate to enforce or defend our intellectual property rights against infringement and unauthorized use by competitors, and to protect our trade secrets. In so doing, we may place our intellectual property at risk of being invalidated, held unenforceable, narrowed in scope or otherwise limited. Further, an adverse result in any litigation or defense proceedings may increase the risk of non-issuance of pending applications. In addition, if any licensor fails to enforce or defend its intellectual property rights, this may adversely affect our ability to develop and commercialize our SPEAR T-cells and to prevent competitors from making, using, and selling competing products. Any such litigation could be very costly and could distract our management from focusing on operating our business. The existence and/or outcome of any such litigation could harm our business, results of operations and financial condition.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential and proprietary information could be compromised by disclosure during this type of litigation. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of our ADSs.
We may not be able to protect our proprietary technology in the marketplace or the cost of doing so may be prohibitive or excessive.
Our success will depend, in part, on our ability to obtain patents, protect our trade secrets and operate without infringing on the proprietary rights of others. We rely upon a combination of patents, trade secret protection (i.e., know-how), and confidentiality agreements to protect the intellectual property of our SPEAR T-cells. The scope and validity of patents in the pharmaceutical field involve complex legal and scientific questions and can be uncertain. Where appropriate, we seek patent protection for certain aspects of our SPEAR T-cells and technology. Filing, prosecuting and defending patents throughout the world would be prohibitively expensive, so our policy is to patent technology in jurisdictions with significant commercial opportunities. However, patent protection may not be available for some of the SPEAR T-cells or technology we are developing. If we must spend significant time and money protecting or enforcing our patents, designing around patents held by others or licensing, potentially for large fees, patents or other proprietary rights held by others, our business results of operations and financial condition may be harmed. We may not develop additional proprietary products that are patentable.
Many companies have encountered significant problems in protecting and enforcing intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents and other intellectual property rights, particularly those relating to pharmaceuticals, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial cost and divert our efforts and attention from other aspects of our business.
58
Table of Contents
In addition, patents have a limited lifespan. In most countries, including the United States, the standard expiration of a patent is 20 years from the effective filing date. Various extensions of patent term may be available in particular countries; however, in all circumstances the life of a patent, and the protection it affords, has a limited term. If we encounter delays in obtaining regulatory approvals, the period of time during which we could market a product under patent protection could be reduced. We expect to seek extensions of patent terms where these are available in any countries where we are prosecuting patents. Such possible extensions include those permitted under the Drug Price Competition and Patent Term Restoration Act of 1984 in the United States, which permits a patent term extension of up to five years to cover an FDA-approved product. The actual length of the extension will depend on the amount of patent term lost while the product was in clinical trials. However, the applicable authorities, including the FDA in the United States, and any equivalent regulatory authority in other countries, may not agree with our assessment of whether such extensions are available, and may refuse to grant extensions to our patents, or may grant more limited extensions than we request. If this occurs, our competitors may be able to take advantage of our investment in development and clinical trials by referencing our clinical and non-clinical data, and then may be able to launch their product earlier than might otherwise be the case.
Any loss of, or failure to obtain, patent protection could have a material adverse impact on our business. We may be unable to prevent competitors from entering the market with products that are similar to or the same as our SPEAR T-cells.
Further given that our technology relates to the field of genetic engineering, political pressure or ethical decisions may result in a change to the scope of patent claims for which we may be eligible. Different patent offices throughout the world may adopt different procedures and guidelines in relation to what is and is not patentable and as a result different protection could be obtained in different areas of the world which may impact our ability to maximize commercialization of our technology.
We may also incur increased expenses and cost in relation to the filing and prosecution of patent applications where third parties choose to challenge the scope or oppose the grant of any patent application or, following grant, seek to limit or invalidate any patent. On April 13, 2015, we received notification of a third party observation filed against one of the patent applications (PCT/GB2013/053320) jointly owned with Immunocore and covering one aspect of our underlying processes. The third party observation cites a reference which the third party considers to be novelty destroying in relation to claims 1-14 of our patent application. Following this observation, an examination report was issued by the patent office and we have responded to the cited observations in the examination report in full. Any increased prosecution or defense required in relation to such patents and patent applications, whether relating to this third party observation or any other third party challenge or opposition, entails increased cost and resource commitment to the business and may result in patents and patent applications being abandoned, invalidated or narrowed in scope.
We may be unable to adequately prevent disclosure of trade secrets and other proprietary information.
We rely on trade secrets to protect our proprietary know-how and technological advances, especially where we do not believe patent protection is appropriate or obtainable. However, trade secrets are difficult to protect. We rely, in part, on confidentiality agreements with our employees, consultants, outside scientific collaborators, sponsored researchers and other advisors to protect our trade secrets and other proprietary information. These agreements may not effectively prevent disclosure of confidential information and may not provide an adequate remedy in the event of unauthorized disclosure of confidential information. In addition, others may independently discover our trade secrets and proprietary information. Costly and time-consuming litigation could be necessary to enforce and determine the scope of our proprietary rights. Failure to obtain or maintain trade secret protection, or failure to adequately protect our intellectual property, could enable competitors to develop generic products or use our proprietary information to develop other products that compete with our SPEAR T-cells or have additional, material adverse effects upon our business, results of operations and financial condition.
In addition, we provide samples to third parties under material transfer agreements, including to research institutions or other organizations that we cannot control. There is a risk that such third parties could disclose details of those samples or carry out further research in relation to provided samples which results in intellectual property rights that block our future freedom to operate, and to which we may not be able to obtain a license on commercially acceptable terms or at all. In addition, provision of samples and our confidential information to such parties could facilitate or assist such parties in development of competing products.
59
Table of Contents
If third parties claim that our activities or products infringe upon their intellectual property, our operations could be adversely affected.
There is a substantial amount of litigation, both within and outside the United States, involving patents and other intellectual property rights in the pharmaceutical industry. We may, from time to time, be notified of claims that we are infringing upon patents, trademarks, copyrights, or other intellectual property rights owned by third parties, and we cannot provide assurances that other companies will not, in the future, pursue such infringement claims against us or any third-party proprietary technologies we have licensed. If we were found to infringe upon a patent or other intellectual property right, or if we failed to obtain or renew a license under a patent or other intellectual property right from a third party, or if a third party that we were licensing technologies from was found to infringe upon a patent or other intellectual property rights of another third party, we may be required to pay damages, including triple damages if the infringement is found to be willful, suspend the manufacture of certain SPEAR T-cells or reengineer or rebrand our SPEAR T-cells, if feasible, or we may be unable to enter certain new product markets. Any such claims could also be expensive and time- consuming to defend and divert management’s attention and resources. Our competitive position could suffer as a result. In addition, if we have declined to enter into a valid non-disclosure or assignment agreement for any reason, we may not own an invention or intellectual property rights and may not be adequately protected. Although we have reviewed certain third-party patents and patent filings that we believe may be relevant to our SPEAR T-cells, we have not conducted a full freedom-to-operate search or analysis for such SPEAR T-cells, and we may not be aware of patents or pending or future patent applications that, if issued, would block us from commercializing our SPEAR T-cells. Thus, we cannot guarantee that we can successfully commercialize SPEAR T-cells in a way that will not infringe any third party’s intellectual property.
Licenses may be required from third parties in relation to any SPEAR T-cells developed or commercialized by us.
We may identify third-party intellectual property rights that are required to enable the further development, commercialization, manufacture or development of our SPEAR T-cells. Licenses to such intellectual property rights may or may not be available on commercial terms that are acceptable to us. As a result we may incur additional license fees for such intellectual property rights, or the cost and expenses to identify an alternative route for commercialization, that does not require the relevant third-party intellectual property rights, or the cost and diversion of resources required to challenge any such third party intellectual property rights.
We have identified three third party European patent applications which relate to high affinity TCR proteins and methods. Two of these patent applications have been amended and the claims are not relevant to our SPEAR T-cell technology. The final application includes broad claims which we do not currently perceive as relevant to our business. We have previously filed third party observations in relation to these claims and have recently filed further third party observations arguing on the basis of lack of support, lack of clarity, disallowed added matter, non-entitlement to priority, and lack of inventive step. Should these patent applications proceed to grant in Europe with claims of broad scope, we may need to consider filing Opposition proceedings against the grant of the European patents at the European Patent Office and/or filing for revocation of the national patents derived from the European patents before relevant national patent offices and/or courts.
We have also identified a family of third party patents under which we may require a license in relation to a structural component of our lentiviral vector (cPPT) prior to any commercialization of SPEAR T-cells. We believe such licenses are available and we are in discussions to procure a license or freedom to operate under the relevant patent rights.
We may also require licenses under third-party patents covering certain peptide sequences or the use of those peptides. Such licenses will require payment of sums by us and we cannot guarantee that the terms of such licenses will be available on commercially acceptable terms or at all, which could limit the peptides which can be used by us and the efficacy of the final affinity- enhanced TCRs that we are able to offer.
As we change, develop and modify our manufacturing processes we may identify further third-party patents covering those developments and modifications. We cannot guarantee that we will be able to obtain licenses under these third-party patents or other intellectual property rights and as a result we may not be able to undertake the developments of modifications that we wish, either at all or in the timescales we require. This could ultimately impact our ability to deliver commercial T-cell products at the cost required.
Further or other third-party patents and patent applications may be identified from time to time that require prospective action by us to prevent the grant of broad claims. Such prospective action requires time and expense and also impacts on the resources generally available to us.
60
Table of Contents
Where we license certain technology from a third party, the prosecution, maintenance and defense of the patent rights licensed from such third party may be controlled by the third party which may impact the scope of patent protection which will be obtained or enforced.
Where we license patent rights or technology from a third-party, control of such third party patent rights may vest in the licensor, particularly where the license is non-exclusive or field restricted. This may mean that we are not able to control or affect the scope of the claims of any relevant third-party patent or have control over any enforcement of such a patent. Where a licensor brings an enforcement action, this could negatively impact our business or result in additional restrictions being imposed on the license we have and the scope of such license, or result in invalidation or limitation of the scope of the licensed patent. In addition, should we wish to enforce the relevant patent rights against a third person, we may be reliant on consent from the relevant licensor or the cooperation of the licensor. The licensor may refuse to bring such action and leave us unable to restrict competitor entry into the market.
Issued patents protecting our SPEAR T-cells could be found invalid or unenforceable if challenged in court or at the USPTO.
If we or one of our licensing partners initiate legal proceedings against a third party to enforce a patent protecting one of our SPEAR T-cells, the defendant could counterclaim that the patent protecting our SPEAR T-cell, as applicable, is invalid and/or unenforceable. In patent litigation in the United States, defendant counterclaims alleging invalidity and/or unenforceability are commonplace, and there are numerous grounds upon which a third party can assert invalidity or unenforceability of a patent. Third parties may also raise similar claims before administrative bodies in the United States or abroad, even outside the context of litigation. Such mechanisms include re-examination, post grant review, and equivalent proceedings in foreign jurisdictions (e.g., opposition proceedings). Such proceedings could result in revocation or amendment to our patents in such a way that they no longer cover our SPEAR T-cells. The outcome following legal assertions of invalidity and unenforceability is unpredictable. With respect to the validity question, for example, we cannot be certain that there is no invalidating prior art, of which we, our patent counsel and the patent examiner were unaware during prosecution. If a defendant were to prevail on a legal assertion of invalidity and/or unenforceability, we would lose at least part, and perhaps all, of the patent protection for our SPEAR T-cells. Such a loss of patent protection could have a material adverse impact our business, financial condition and results of operations.
Changes in U.S. patent law could diminish the value of patents in general, thereby impairing our ability to protect our products.
As is the case with other biopharmaceutical companies, our success is heavily dependent on intellectual property, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involve both technological and legal complexity, and is therefore costly, time-consuming and inherently uncertain. In addition, the United States has recently enacted and is currently implementing wide-ranging patent reform legislation. Recent U.S. Supreme Court rulings have narrowed the scope of patent protection available in certain circumstances and weakened the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained. Depending on decisions by the U.S. Congress, the federal courts, and the USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future. For example, in the recent case, Assoc. for Molecular Pathology v. Myriad Genetics, Inc., the U.S. Supreme Court held that certain claims to DNA molecules are not patentable. While we do not believe that any of the patents owned or licensed by us will be found invalid based on this decision, we cannot predict how future decisions by the courts, the U.S. Congress or the USPTO may impact the value of our patents.
Our ability to protect our intellectual property rights in territories outside of the United States may vary and thus affect our ability to obtain revenue from our SPEAR T-cells.
Filing, prosecuting and defending patents on our SPEAR T-cells in all countries throughout the world would be prohibitively expensive, and the extent of intellectual property rights may be less extensive than those which can be obtained in the United States. Consequently, we may not be able to prevent third parties from practicing our inventions in all countries outside the United States, or from selling or importing products made using our inventions in and into the United States or other jurisdictions. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and further, may export otherwise infringing products to territories where we have patent protection, but enforcement is not as strong as that in the United States. These products may compete with our products and our patents or other intellectual property rights may not be effective or sufficient to prevent them from competing.
61
Table of Contents
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents, trade secrets and other intellectual property protection, particularly those relating to biopharmaceutical products, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or license.
Risks Related to Employee Matters and Managing Growth
We depend upon our key personnel and our ability to attract and retain employees.
We are heavily dependent on the ongoing employment and involvement of certain key employees in particular, James Noble, our Chief Executive Officer, Dr. Helen Tayton-Martin, our Chief Operating Officer, Dr. Rafael Amado, our Chief Medical Officer, Dr. Gwendolyn Binder-Scholl, our Chief Technology Officer, and Adrian Rawcliffe, our Chief Financial Officer. We do not hold key-man insurance for our senior managers. In addition, James Noble and Dr. Helen Tayton-Martin, are in a personal relationship. They are our co-founders, two of our most senior executive officers and are a vital part of our business. If the personal relationship ended or they could otherwise not amicably work with each other, one of them may decide to leave us which would materially harm our business.
In addition, we anticipate a requirement to expand the personnel available to us very rapidly in order to achieve our planned business activities and aims. Such expansion is dependent on our ability to recruit experienced and suitably trained employees or consultants, and to retain such employees on a long term basis. Our ability to take our existing pipeline of TCR therapeutics and to meet the demands of the GSK collaboration may be compromised or delayed where we are unable to recruit sufficient personnel on a timely basis.
To induce employees to remain at our company, in addition to salary and cash incentives, we have provided share options that vest over time, with higher awards of share options being made to senior employees. The value to employees of share options that vest over time may be significantly affected by movements in our share price that are beyond our control, and may at any time be insufficient to counteract more lucrative offers from other companies. Despite our efforts to retain valuable employees, members of our management, scientific and development teams may terminate their employment with us on short notice. Although we have employment agreements with all of our employees, in the United Kingdom, these employment agreements provide for a mutual nine months’ notice period in the case of Mr. Noble, a mutual six months’ notice period in the case of Dr. Tayton-Martin; mutual three months’ notice periods in the case of senior managers and mutual one month notice periods for all other employees. In the United States, the employment agreements provide for at-will employment except that, under their employment agreements, Dr. Amado, Dr. Binder-Scholl and Mr. Rawcliffe must provide 60 days’ written notice for termination without cause. This means that any of our employees in the United States, except for Dr. Amado, Dr. Binder-Scholl and Mr. Rawcliffe, could leave our employment at any time, with or without notice. Our success also depends on our ability to continue to attract, retain and motivate highly skilled junior, mid-level and senior managers as well as junior, mid-level and senior scientific and medical personnel.
We will need to grow the size and capabilities of our organization, and we may experience difficulties in managing this growth.
As of December 31, 2016, we had 298 full-time equivalent employees. As our development and commercialization plans and strategies develop, we must add a significant number of additional managerial, operational, sales, marketing, financial, and other personnel. Future growth will impose significant added responsibilities on members of management, including:
· identifying, recruiting, integrating, maintaining, and motivating additional employees;
· managing our internal development efforts effectively, including the clinical and FDA review process for our SPEAR T-cells, while complying with our contractual obligations to contractors and other third parties; and
· improving our operational, financial and management controls, reporting systems, and procedures.
Our future financial performance and our ability to commercialize our SPEAR T-cells will depend, in part, on our ability to effectively manage any future growth, and our management may also have to divert a disproportionate amount of its attention away from day-to-day activities in order to devote a substantial amount of time to managing these growth activities.
We also rely on third parties to provide certain of our manufacturing and quality capabilities. See “Risks Related to Our Reliance Upon Third Parties.”
62
Table of Contents
If we are not able to effectively expand our organization by hiring new employees and expanding our groups of consultants and contractors, we may not be able to successfully implement the tasks necessary to further develop and commercialize our SPEAR T-cells and, accordingly, may not achieve our research, development, and commercialization goals.
Expansion of our business has necessitated a move in premises both in the United Kingdom and in the United States. While the move in the United States has occurred, work is still ongoing to enable operation as a manufacturing facility. The move in the United Kingdom is due to occur in mid-2017 and will cause interruption to our research and development work, including pre-clinical safety testing. The move requires transfer of all equipment, cell lines, tissues and materials to the new premises and re-validation and calibration of equipment. Any failure to properly validate or calibrate equipment or any destruction of materials transferred to the new premises may result in additional delays to the work carried out in the United Kingdom.
We are intending to open a manufacturing facility of our own which may be delayed or which may result in increased costs being incurred by the company
We are in the process of development a manufacturing facility for our SPEAR T-cell products within our Navy Yard facility in Philadelphia, United States. As a company we have never operated our own manufacturing facility or manufactured SPEAR T-cells ourselves. The ability to use the Navy Yard facility for manufacture of our products within a reasonable period of time is dependent on a number of factors including:
· our ability to recruit the required employees at a suitable level and experience;
· our ability to obtain regulatory approval for the facility and for SPEAR T-cells manufactured at the facility and to satisfy regulatory authorities on an ongoing basis;
· our ability to develop internal quality controls and processes sufficient to enable manufacture and supply of SPEAR T-cells at our Navy Yard facility;
· our ability to establish comparability with currently used manufacturing processes;
· our ability to be able to fund the ongoing development including equipment requirements necessary for successful manufacture of SPEAR T-cells at our facility.
Should we be unable to successfully start manufacture of SPEAR T-cells at our facility within the timescales currently anticipated this could result in delays to the supply of SPEAR T-cells for our clinical programs. Should any of our third party manufacturers cease to be able to supply SPEAR T-cells prior to the time at which our manufacturing facility is able to produce SPEAR T-cells for use in our clinical programs, then we will be unable to support such clinical programs until alternative manufacturing capability is secured. The cost of developing, out-fitting and running a manufacturing facility may also be greater than currently anticipated and we may require additional capital for the completion of the manufacturing facility which may result in the need for us to raise additional funds earlier than expected.
We expect to face intense competition, often from companies with greater resources and experience than we have.
Immunotherapy is an intensely competitive area with many of the large pharmaceutical companies having products and therapies already in clinical trials for cancer indications and autoimmune diseases. The larger resources of these companies may enable them to take therapies all the way through the regulatory process, while we will require additional investment or input from collaborators such as GSK to take our SPEAR T-cells through the regulatory process and commercialization. Smaller or early-stage companies may also prove to be significant competitors, particularly if such companies align with pharmaceutical partners and compete for patients. Results obtained by such competitors in clinical trials could also impact our ability to obtain regulatory approval or delay such approval in the event of a safety issue or other negative clinical result associated with similar T-cell or SPEAR T-cells.
In particular, we face competition from chimeric antigen receptor T-cell, or CAR-T, technologies from companies such as Novartis AG/University of Pennsylvania, Kite Pharma, Inc./Amgen Inc./National Cancer Institute, bluebird bio, Inc./Celgene Corporation/Baylor College of Medicine, Intrexon Corporation/Ziopharm Oncology, Inc./MD Anderson Cancer Center, Juno Therapeutics, Inc./Celgene Corporation/Fred Hutchinson Cancer Research Center/Memorial Sloan Kettering Cancer Center, Cellectis SA/Pfizer Inc./Servier Laboratories and Bellicum Pharmaceuticals Inc. In the TCR space, we face competition from Juno Therapeutics, Inc., Kite Pharma, Inc., Medigene AG/Bluebird Bio Inc., Bellicum Pharmaceuticals Inc., Cell Therapy TCR Ltd., Eureka Therapeutics Inc., and Takara Bio, Inc. Kite Pharma, Inc. has a murine derived TCR product in pre-clinical development targeting NY-ESO-1 and Takara Bio, Inc. have TCR product candidates in early clinical studies targeting NY-ESO-1 and MAGE-A4. Medigene AG has reported development of a PRAME TCR therapeutic candidate and is collaborating on a MAGE-A1 TCR which is due to enter clinical trials later in 2017. Eureka Therapeutics Inc. has announced the development of CAR-T products which target peptide-HLA complexes. They have developed CAR-Ts targeting the same NY-ESO and AFP peptides as are targeted by our SPEAR T-cells. However development still appears to be in the early stages and limited data is available to assess impact on our own SPEAR T-cells, if any. Ziopharm Oncology, Inc. has announced the development of a TCR mimetic CAR-T targeting NY-ESO-1. Adicet Bio/Regeneron Inc. have announced plans to develop TCR immunotherapy products directed to MHC-peptide complexes and Tactiva Therapeutics are developing CD4-TCRs and CD8-TCRs targeting solid tumors expressing NY-ESO. Should Kite Pharma, Inc., Takara Bio, Inc. or any of our other competitors be successful in advancing a TCR product targeting NY-ESO-1 through development,
63
Table of Contents
our ability to develop and advance our NY-ESO SPEAR T-cell could be adversely affected. We may also face competition from other non-TCR and non-cell based treatments such as antibody and check point inhibitor therapies offered by companies such as Amgen Inc., AstraZeneca plc, Bristol-Myers Squibb Company, Incyte Corporation, Merck & Co., Inc., and Roche Holding Ltd. Even if we obtain regulatory approval for our SPEAR T-cells, we may not be the first to market, which could affect both demand for and price of our SPEAR T-cells.
Although Immunocore is focused on soluble TCRs rather than engineered SPEAR T-cells, we could also face competition from Immunocore if it develops or acquires products directed at the same targets or indications as our TCR therapeutic product candidates.
Moreover, many of our employees have come from a shared background within Immunocore and there is an awareness within Immunocore of certain of our confidential information on the technology platform controlled through confidentiality agreements. This knowledge could be used by Immunocore to facilitate its own developments or to target competitive products against our products placing it in a preferable position as compared to third party competitors.
The results of the United Kingdom’s referendum on withdrawal from the European Union may have a negative effect on global economic conditions, financial markets and our business.
On June 23, 2016, a majority of voters in the United Kingdom elected to withdraw from the European Union in a national referendum. The terms of any withdrawal are subject to a negotiation period that could last at least two years after the government of the United Kingdom formally initiates a withdrawal process. Nevertheless, the referendum has created significant uncertainty about the future relationship between the United Kingdom and the European Union, including with respect to the laws and regulations that will apply as the United Kingdom determines which European Union laws to replace or replicate in the event of a withdrawal. The referendum has also given rise to calls for the governments of other European Union member states to consider withdrawal. These developments, or the perception that any of them could occur, may have a material adverse effect on global economic conditions and the stability of global financial markets, and may significantly reduce global market liquidity and restrict the ability of key market participants to operate in certain financial markets. Any of these factors could depress economic activity and restrict our access to capital, which could have a material adverse effect on our business, financial condition and results of operations and reduce the price of our securities. In addition, currency exchange rates in the pounds sterling and the euro with respect to each other and the U.S. dollar have already been adversely affected by these developments. Should this foreign exchange volatility continue, it could cause volatility in our quarterly financial results which may affect the market price of our ADSs.
Failure of our information technology systems could significantly disrupt the operation of our business.
Our ability to execute our business plan and to comply with regulators’ requirements with respect to data control and data integrity, depends, in part, on the continued and uninterrupted performance of our information technology systems and similar systems used by third-party providers that we rely on. These systems are vulnerable to damage from a variety of sources, including telecommunications or network failures, malicious human acts and natural disasters. Moreover, despite network security and back-up measures, some of our servers are potentially vulnerable to physical or electronic break-ins, computer viruses and similar disruptive problems. Despite the precautionary measures we have taken to prevent unanticipated problems that could affect our information systems, sustained or repeated system failures or problems arising during the upgrade of any of our information systems that interrupt our ability to generate and maintain data, and in particular to operate our proprietary technology platform, could adversely affect our ability to operate our business. In addition, where disruption to such systems occurs at third-party providers, we may have limited ability to find alternative providers in any required timeframes or at all, and such disruption could significantly affect our ability to proceed with clinical or analytical or development programs.
Business disruptions could seriously harm our future revenue and financial condition and increase our costs and expenses.
Our operations and those of our third party suppliers and collaborators could be subject to earthquakes, power shortages, telecommunications failures, water shortages, floods, hurricanes or other extreme weather conditions, medical epidemics, labor disputes or other business interruptions. While the company has business interruption insurance policies in place, any interruption could seriously harm our ability to timely proceed with any clinical programs or to supply SPEAR T-cells on a commercial basis or for use in clinical programs.
64
Table of Contents
We are exposed to risks related to currency exchange rates.
We conduct a significant portion of our operations within the United Kingdom in both U.S. dollars and pounds sterling and our arrangements with GSK are denominated in pounds sterling. Changes in currency exchange rates have had and could have a significant effect on our operating results. Exchange rate fluctuations between the U.S. dollar and local currencies create risk in several ways, including the following: weakening of the pound sterling may increase the cost of overseas research and development expenses and other costs outside the United Kingdom; strengthening of the U.S. dollar may decrease the value of any future revenues denominated in other currencies. Effects of exchange rates on transactions and cash deposits held in a currency other than the functional currency of a subsidiary can distort our financial results; and commercial pricing and profit margins are affected by currency fluctuations.
We may be classified as a passive foreign investment company in any taxable year and U.S. holders of our ADSs could be subject to adverse U.S. federal income tax consequences.
The rules governing passive foreign investment companies, or PFICs, can have adverse effects for U.S. federal income tax purposes. The tests for determining PFIC status for a taxable year depend upon the relative values of certain categories of assets and the relative amounts of certain kinds of income. The determination of whether we are a PFIC depends on the particular facts and circumstances (such as the valuation of our assets, including goodwill and other intangible assets) and may also be affected by the application of the PFIC rules, which are subject to differing interpretations. Based on our estimated gross income, the average value of our assets, including goodwill and the nature of our active business, we do not believe that the Company was classified as a PFIC for U.S. federal income tax purposes for the U.S. taxable year ended December 31, 2016. There can be no assurance, however, that we will not be considered to be PFIC for any particular year in the future because PFIC status is factual in nature, depends upon factors not wholly within our control, generally cannot be determined until the close of the taxable year in question, and is determined annually.
If we are a PFIC, U.S. holders of our ADSs would be subject to adverse U.S. federal income tax consequences, such as ineligibility for any preferred tax rates on capital gains or on actual or deemed dividends, interest charges on certain taxes treated as deferred, and additional reporting requirements under U.S. federal income tax laws and regulations. A U.S. holder of our ADSs may be able to mitigate some of the adverse U.S. federal income tax consequences described above with respect to owning the ADSs if we are classified as a PFIC, provided that such U.S. investor is eligible to make, and validly makes, a “mark-to-market” election. In certain circumstances a U.S. Holder can make a “qualified electing fund” election to mitigate some of the adverse tax consequences described with respect to an ownership interest in a PFIC by including in income its share of the PFIC’s income on a current basis. However, we do not currently intend to prepare or provide the information that would enable a U.S. Holder to make a qualified electing fund election.
Investors should consult their own tax advisors regarding all aspects of the application of the PFIC rules to our ordinary shares.
Risks Related to Ownership of our American Depositary Shares (ADSs)
The price of our ADSs may be volatile.
Many factors may have a material adverse effect on the market price of the ADSs, including but not limited to:
· the commencement, enrollment or results of our planned clinical trials;
· the loss of any of our key scientific or management personnel;
· announcements of the failure to obtain regulatory approvals or receipt of a complete response letter from the FDA;
· announcements of undesirable restricted labeling indications or patient populations, or changes or delays in regulatory review processes;
· announcements of therapeutic innovations or new products by us or our competitors;
· adverse actions taken by regulatory agencies with respect to our clinical trials, manufacturing supply chain or sales and marketing activities;
· changes or developments in laws or regulations applicable to our SPEAR T-cells;
· any adverse changes to our relationship with licensors, manufacturers or suppliers;
65
Table of Contents
· the failure of our testing and clinical trials;
· unanticipated safety concerns;
· the failure to retain our existing, or obtain new, collaboration partners;
· announcements concerning our competitors or the pharmaceutical industry in general;
· the achievement of expected product sales and profitability;
· the failure to obtain reimbursements for our SPEAR T-cells, if approved for marketing, or price reductions;
· manufacture, supply or distribution shortages;
· actual or anticipated fluctuations in our operating results;
· our cash position;
· changes in financial estimates or recommendations by securities analysts;
· potential acquisitions;
· the trading volume of ADSs on Nasdaq;
· sales of our ADSs by us, our executive officers and directors or our shareholders in the future;
· general economic and market conditions and overall fluctuations in the U.S. equity markets;
· the change in our status from reporting as a foreign private issuer to reporting as a U.S. domestic company now using Securities Act and Exchange Act U.S. domestic company forms; and
· changes in accounting principles.
In addition, the stock market in general, and Nasdaq and biopharmaceutical companies in particular, have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of these companies. Broad market and industry factors may negatively affect the market price of our ADSs, regardless of our actual operating performance. Further, a decline in the financial markets and related factors beyond our control may cause the price of our ADSs to decline rapidly and unexpectedly.
Substantial future sales of our ADSs in the public market, or the perception that these sales could occur, could cause the price of the ADSs to decline and dilute shareholders.
Substantial future sales of our ADSs in the public market, or the perception that these sales could occur, could cause the market price of the ADSs to decline. Each ADS represents six ordinary shares and 11,250,000 ADSs, representing 67,500,000 ordinary shares, have been freely transferable without restriction or additional registration under the U.S. Securities Act of 1933, as amended (the “Securities Act”), since our IPO. The remaining 357,211,900 ordinary shares were subject to a lock-up period, which expired on November 1, 2015. Subsequent to the expiration of the lock-up, and following conversion into ADSs, these shares have been available for sale subject to volume limitations and other restrictions as applicable under Rule 144 under the Securities Act. To the extent these shares are sold into the market, particularly in substantial quantities, the market price of our ADSs could decline.
We also entered into a registration rights agreement on February 23, 2015, pursuant to which we have agreed, under certain circumstances, to file a registration statement to register the resale of the shares held by certain of our existing shareholders, as well as to cooperate in certain public offerings of such shares. In addition, we have registered an aggregate of 66,999,747 ordinary shares that we may issue under our equity compensation plans and, as a result, they can be freely sold in the public market upon issuance and following conversion into ADSs, but subject to volume limitations applicable to affiliates under Rule 144. Additionally, the majority of ordinary shares that may be issued under our equity compensation plans also remain subject to vesting in tranches over a four year period. As of December 31, 2016, an aggregate of 17,167,347 options over our ordinary shares had vested and become exercisable. If a large number of our ADSs are sold in the public market after they become eligible for sale, the sales could reduce the trading price of our ADSs and impede our ability to raise future capital.
66
Table of Contents
Our decision to report under the regime applicable to U.S. domestic issuers earlier than required has led to higher legal, accounting and other related expenses than we incurred when we reported as a foreign private issuer and we expect to continue to incur increased expenses.
We had determined that we would be required to use the forms and follow the reporting requirements for a U.S. domestic issuer beginning on January 1, 2017. However, we decided to voluntarily switch to the U.S. domestic issuer forms effective from January 1, 2016 and also changed our fiscal year to a calendar year, all with the goals of aligning our fiscal reporting more closely with comparable companies in the industry which use calendar years, report under U.S. GAAP and generally file on the U.S. domestic forms. We have incurred significant legal, accounting and other expenses as we have adjusted to reporting in U.S. dollars and under U.S. GAAP and following the form and substantive accounting and disclosure requirements applicable to U.S. domestic issuers. We expect to continue to incur higher costs associated with reporting under the regime applicable to U.S domestic issuers than when we reported as a foreign private issuer.
We are an emerging growth company and we cannot be certain that the reduced disclosure requirements applicable to emerging growth companies will not make our ADSs less attractive to investors.
We are an “emerging growth company,” as defined in the Jumpstart Our Business Start-ups Act of 2012, or the JOBS Act, and have elected to take advantage of the following provisions of the JOBS Act: the exemption from the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act; not providing all of the compensation disclosure that may be required of non-emerging growth public companies under the U.S. Dodd-Frank Wall Street Reform and Consumer Protection Act; not disclosing certain executive compensation-related items such as the correlation between executive compensation and performance and comparisons of the Chief Executive Officer’s compensation to employee compensation; not complying with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements (auditor discussion and analysis and an extended transition period to comply with new or revised accounting standards applicable to public companies). In addition, to the extent that we no longer qualify as a foreign private issuer, we have elected to take advantage of (1) reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements; and (2) exemptions from the requirements of holding a non-binding advisory vote on executive compensation including golden parachute compensation. As a result of these elections, our future financial statements may not be comparable to companies that comply with these obligations earlier and our investors may not have access to certain information they may deem important.
Our independent registered public accounting firm will not be required to provide an attestation report on the effectiveness of our internal control over financial reporting as long as we qualify as an “emerging growth company,” which may increase the risk that weaknesses or deficiencies in our internal control over financial reporting go undetected and may make it more difficult for investors and securities analysts to evaluate our company. We may take advantage of these reporting exemptions until we are no longer an emerging growth company. We will remain an emerging growth company until the earliest of (i) the last day of the fiscal year in which we have total annual gross revenue of $1.0 billion or more; (ii) the last day of our fiscal year following the fifth anniversary of May 6, 2015, the date our ADSs began trading; (iii) the date on which we have issued more than $1.0 billion in nonconvertible debt during the previous three years; and (iv) the date on which we are deemed to be a large accelerated filer under the rules of the SEC. We cannot predict if investors will find our ADSs less attractive because we may rely on these exemptions. If some investors find our ADSs less attractive, there may be a less active trading market for our ADSs, and the price of our ADSs may be more volatile and may decline.
If we fail to establish and maintain proper internal controls, our ability to produce accurate financial statements or comply with applicable regulations could be impaired.
Section 404(a) of the Sarbanes-Oxley Act, requires that beginning with our second annual report following our IPO, management assess and report annually on the effectiveness of our internal controls over financial reporting and identify any material weaknesses in our internal controls over financial reporting. Although Section 404(b) of the Sarbanes-Oxley Act requires our independent registered public accounting firm to issue an annual report that addresses the effectiveness of our internal controls over financial reporting, we have opted to rely on the exemptions provided in the JOBS Act, and consequently will not be required to comply with SEC rules that implement Section 404(b) of the Sarbanes-Oxley Act until such time as we are no longer an emerging growth company.
67
Table of Contents
Our first Section 404(a) assessment took place for our annual report for our fiscal year ending December 31, 2016. The presence of material weaknesses could result in financial statement errors which, in turn, could lead to errors in our financial reports, delays in our financial reporting, could require us to restate our operating results or our auditors may be required to issue a qualified audit report. We might not identify one or more material weaknesses in our internal controls in connection with evaluating our compliance with Section 404(a) of the Sarbanes-Oxley Act. In order to maintain and improve the effectiveness of our disclosure controls and procedures and internal controls over financial reporting, we will need to expend significant resources and provide significant management oversight. Implementing any appropriate changes to our internal controls may require specific compliance training of our directors and employees, entail substantial costs in order to modify our existing accounting systems, take a significant period of time to complete and divert management’s attention from other business concerns. These changes may not, however, be effective in maintaining the adequacy of our internal control.
If either we are unable to conclude that we have effective internal controls over financial reporting or, at the appropriate time, our independent auditors are unwilling or unable to provide us with an unqualified report on the effectiveness of our internal controls over financial reporting as required by Section 404(b) of the Sarbanes-Oxley Act, investors may lose confidence in our operating results, the price of our ADSs could decline and we may be subject to litigation or regulatory enforcement actions. In addition, if we are unable to meet the requirements of Section 404 of the Sarbanes-Oxley Act, we may not be able to remain listed on Nasdaq.
We incur significant increased costs as a result of operating as a company whose ADSs are publicly traded in the United States, and our management is required to devote substantial time to new compliance initiatives.
As a company whose ADSs are publicly traded in the United States since May 6, 2015, we have incurred, and will continue to incur, significant legal, accounting, insurance and other expenses that we did not previously incur as a private company. In addition, the Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Consumer Protection Act and related rules implemented by the SEC and Nasdaq have imposed various requirements on public companies including requiring establishment and maintenance of effective disclosure and financial controls. Our management and other personnel need to devote a substantial amount of time to these compliance initiatives. Moreover, these rules and regulations have increased, and will continue to increase, our legal and financial compliance costs and will make some activities more time-consuming and costly. Our insurance costs have increased, particularly for directors and officers liability insurance, and we may be required to incur further substantial increased costs to maintain the same or similar coverage or be forced to accept reduced coverage in future. These laws and regulations could also make it more difficult and expensive for us to attract and retain qualified persons to serve on our board of directors, our board committees or as our executive officers. Furthermore, if we are unable to satisfy our obligations as a public company, we could be subject to delisting of the ADSs from Nasdaq, fines, sanctions and other regulatory action and potentially civil litigation.
U.S. investors may have difficulty enforcing civil liabilities against our company, our directors, officers and members of senior management.
We are incorporated under the laws of England and Wales. The rights of holders of our ordinary shares and, therefore, certain of the rights of holders of ADSs, are governed by English law, including the provisions of the Companies Act 2006, and by our articles of association. These rights differ in certain respects from the rights of shareholders in typical U.S. corporations organized in, for example, Delaware. Some of our directors, officers and members of senior management reside outside the United States, and a substantial portion of our assets and all or a substantial portion of the assets of such persons are located outside the United States. As a result, it may be difficult for you to serve legal process on us or our directors and executive officers or have any of them appear in a U.S. court. The United States and the United Kingdom do not currently have a treaty providing for the recognition and enforcement of judgments, other than arbitration awards, in civil and commercial matters. The enforceability in the United Kingdom of any judgment of a U.S. federal or state court will depend on the particular facts of the case as well as the laws and any treaties in effect at the time, including conflicts of laws principles (such as those bearing on the question of whether a U.K. court would recognize the basis on which a U.S. court had purported to exercise jurisdiction over a defendant). In this context, there is doubt as to the enforceability in the United Kingdom, in original actions or in actions for enforcement of judgments of U.S. courts, of civil liabilities based solely on the federal securities laws of the United States. In addition, awards for punitive damages in actions brought in the United States or elsewhere may be unenforceable in the United Kingdom. An award for monetary damages under the U.S. securities laws would likely be considered punitive if it did not seek to compensate the claimant for loss or damage suffered and was intended to punish the defendant.
68
Table of Contents
Provisions in the U.K. City Code on Takeovers and Mergers may have anti-takeover effects that could discourage an acquisition of us by others, even if an acquisition would be beneficial to our shareholders.
The U.K. City Code on Takeovers and Mergers, or the Takeover Code, applies to an offer for, among other things, a public company whose registered office is in the United Kingdom (or the Channel Islands or the Isle of Man) and whose securities are not admitted to trading on a regulated market or multilateral trading facility in the United Kingdom (or the Channel Islands or the Isle of Man) if the company is considered by the Panel on Takeovers and Mergers, or the Takeover Panel, to have its place of central management and control in the United Kingdom (or the Channel Islands or the Isle of Man). This is known as the “residency test.” The test for central management and control under the Takeover Code is different from that used by the U.K. tax authorities. Under the Takeover Code, the Takeover Panel will determine whether we have our place of central management and control in the United Kingdom by looking at various factors, including the structure of our Board, the functions of the directors and where they are resident.
If at the time of a takeover offer the Takeover Panel considers that we have our place of central management and control in the United Kingdom, we would be subject to a number of rules and restrictions, including but not limited to the following: (1) our ability to enter into deal protection arrangements with a bidder would be extremely limited;(2) we might not, without the approval of our shareholders, be able to perform certain actions that could have the effect of frustrating an offer, such as issuing shares or carrying out acquisitions or disposals; and (3) we would be obliged to provide equality of information to all bona fide competing bidders.
Item 1B. Unresolved Staff Comments
None.
69
Table of Contents
Item 2. Properties
The following table summarizes the facilities we lease as of December 31, 2016, including the location and size of the facilities, and their primary use.
|
Location |
|
Approximate Square Feet |
|
Primary Usage |
|
Lease Expiration Dates |
|
Abingdon, Oxfordshire, United Kingdom |
|
9,738 |
|
Corporate headquarters, Administration |
|
June 2025 |
|
|
|
|
|
|
|
|
|
Abingdon, Oxfordshire, United Kingdom |
|
30,223 |
|
Research, Development, Process development |
|
June 2017 |
|
|
|
|
|
|
|
|
|
Abingdon, Oxfordshire, United Kingdom |
|
67,140 |
|
Research, Development, Process development, Manufacturing, Administration |
|
October 2041 |
|
|
|
|
|
|
|
|
|
Philadelphia, Pennsylvania, United States |
|
47,700 |
|
Manufacturing, Process Development, Research |
|
October 2031 |
|
|
|
|
|
|
|
|
|
Philadelphia, Pennsylvania, United States |
|
29,773 |
|
Administrative, Development |
|
February 2017 |
As of December 31, 2016, all of the above sites were utilized by the Company with the exception of:
· our facilities in Philadelphia, Pennsylvania of 47,700 sq ft, which were occupied in January 2017 following the completion of an internal fit-out; and
· our facilities in Abingdon, Oxfordshire, of 67,140 sq ft, which are undergoing an internal fit-out and are expected to be occupied in the first half of 2017.
In January 2017, we vacated our facilities in Philadelphia, of 29,773 sq ft in order to move to our facilities of 47,700 sq ft. In the first half of 2017, we intend to vacate our facilities in Oxfordshire, of 30,223 sq ft and of 9,738 sq ft in order to move to our facilities of 67,140 sq ft.
We believe that our existing facilities (including our new manufacturing and office facilities in the United Kingdom and United States) are adequate for our near-term needs, but we expect to need additional space as we grow and expand our operations. We believe that suitable additional or alternative office, laboratory, and manufacturing space will be available as required in the future on commercially reasonable terms.
Item 3. Legal Proceedings
As of December 31, 2016, we were not a party to any material legal proceedings.
Item 4. Mine Safety Disclosures
Not applicable
70
Table of Contents
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
The Company’s ordinary shares, par value £0.001 per share, are not publicly traded. The Company’s American Depositary Shares (“ADSs”) each represents six ordinary shares of Adaptimmune Therapeutics plc. An ADS is evidenced by an American Depositary Receipt (“ADR”) issued by Citibank, N.A. as depositary, and is listed on the NASDAQ Global Select Market.
The ADS have been listed on The NASDAQ Global Select Market under the symbol “ADAP” since May 6, 2015. Prior to that date, there was no public trading market for our ADSs or our ordinary shares. Our initial public offering was priced at $17.00 per ADS on May 5, 2015.
The following table sets forth for the periods indicated the high and low intra-day sales prices per ADS as reported on the NASDAQ Global Select Market:
|
|
|
High |
|
Low |
|
|
2016: |
|
|
|
|
|
|
Fourth Quarter |
|
$ |
6.97 |
|
$ |
3.76 |
|
|
Third Quarter |
|
9.13 |
|
6.62 |
|
|
Second Quarter |
|
11.12 |
|
8.02 |
|
|
First Quarter |
|
12.29 |
|
6.52 |
|
|
2015: |
|
|
|
|
|
|
Fourth Quarter |
|
$ |
13.12 |
|
$ |
7.28 |
|
|
Third Quarter |
|
20.24 |
|
10.96 |
|
|
Second Quarter (from May 6, 2015) |
|
21.12 |
|
14.81 |
|
Holders of Common Stock
As of March 8, 2017, there were approximately 31 holders of record of our ordinary shares, par value £0.001 per share, and four holders of record of our ADSs. The closing sales price per ADS on the NASDAQ Global Select Market on March 8, 2017 was $4.24.
Dividends
Since our inception, we have not declared or paid any dividends on our ordinary shares. We intend to retain any earnings for use in our business and do not currently intend to pay dividends on our ordinary shares.
The payment of dividends by Adaptimmune Therapeutics plc is governed by U.K. law. The declaration and payment of any future dividends will be at the discretion of our board of directors and will depend upon our results of operations, cash requirements, financial condition, contractual restrictions, restrictions imposed by our indebtedness, any future debt agreements or applicable laws and other factors that our board of directors may deem relevant.
71
Table of Contents
Performance Graph
This performance graph shall not be deemed “filed” for purposes of Section 18 of the Exchange Act, or incorporated by reference into any of our filings under the Securities Act or the Exchange Act, except as shall be expressly set forth by specific reference in such filing.
The following graph shows the cumulative total stockholder return of an investment of $100 in cash at market close on May 6, 2015 (the first day of trading of our ADSs) through December 31, 2016 for (1) our ADSs, (2) the NASDAQ Composite Index (U.S.) and (3) the NASDAQ Biotechnology Index.
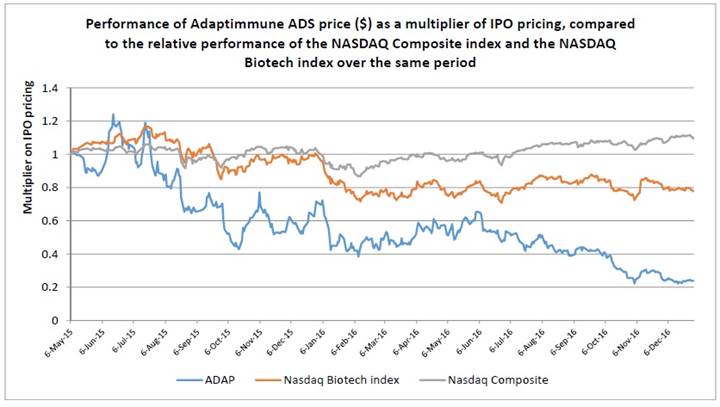
Recent Sales of Unregistered Securities
We did not sell any unregistered securities during the year ended December 31, 2016.
72
Table of Contents
Item 6. Selected Financial Data
The selected statements of operations data for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015, 2014 and 2013 and the selected balance sheet data as of December 31, 2016 and 2015 and June 30, 2015, 2014 and 2013 are derived from our financial statements appearing elsewhere in this Annual Report.
The following selected financial data (in thousands, except for share and per share amounts) should be read in conjunction with the section titled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and the financial statements and related notes appearing elsewhere in this Annual Report. Our historical results are not necessarily indicative of the results that can be expected in the future.
|
|
|
Period ended |
|
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
June 30,
2014 |
|
June 30,
2013 |
|
|
Statements of Operations Data(2): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revenue |
|
$ |
14,198 |
|
$ |
8,979 |
|
$ |
9,871 |
|
$ |
825 |
|
$ |
— |
|
|
Research and development(3) |
|
(63,789 |
) |
(25,472 |
) |
(24,137 |
) |
(9,575 |
) |
(7,273 |
) |
|
General and administrative(3) |
|
(23,208 |
) |
(9,917 |
) |
(10,375 |
) |
(2,771 |
) |
(1,476 |
) |
|
Total operating expenses |
|
(86,997 |
) |
(35,389 |
) |
(34,512 |
) |
(12,346 |
) |
(8,749 |
) |
|
Operating loss |
|
(72,799 |
) |
(26,410 |
) |
(24,641 |
) |
(11,521 |
) |
(8,749 |
) |
|
Interest income |
|
1,110 |
|
489 |
|
504 |
|
— |
|
— |
|
|
Other income (expense), net |
|
1,002 |
|
2,866 |
|
2,323 |
|
(5 |
) |
9 |
|
|
Loss before tax |
|
(70,687 |
) |
(23,055 |
) |
(21,814 |
) |
(11,526 |
) |
(8,740 |
) |
|
Income taxes |
|
(892 |
) |
55 |
|
(244 |
) |
(75 |
) |
— |
|
|
Loss for the year |
|
(71,579 |
) |
(23,000 |
) |
(22,058 |
) |
(11,601 |
) |
(8,740 |
) |
|
Deemed dividends |
|
— |
|
— |
|
(14,735 |
) |
— |
|
— |
|
|
Net loss attributable to ordinary shareholders |
|
(71,579 |
) |
(23,000 |
) |
(36,793 |
) |
(11,601 |
) |
(8,740 |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Basic and diluted loss per share |
|
$ |
(0.17 |
) |
$ |
(0.05 |
) |
$ |
(0.17 |
) |
$ |
(0.08 |
) |
$ |
(0.34 |
) |
|
Weighted average number of shares outstanding(1) |
|
424,713,997 |
|
424,711,900 |
|
214,704,593 |
|
148,335,529 |
|
25,893,846 |
|
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
June 30,
2014 |
|
|
Balance Sheet Data(2): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
158,779 |
|
$ |
194,263 |
|
$ |
229,046 |
|
$ |
51,179 |
|
|
Short-term deposits |
|
22,694 |
|
54,620 |
|
55,292 |
|
— |
|
|
Total assets |
|
234,515 |
|
285,821 |
|
300,653 |
|
55,735 |
|
|
Total liabilities |
|
68,373 |
|
50,828 |
|
41,650 |
|
52,778 |
|
|
Total stockholders’ equity |
|
166,142 |
|
234,993 |
|
259,003 |
|
2,957 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(1) Adjusted to reflect a 1 for 100 stock split effective February 2015.
(2) On April 1, 2015, the Company completed a corporate reorganization. Prior to the corporate reorganization, our business was conducted by Adaptimmune Limited and its consolidated subsidiary. Subsequent to the corporate reorganization, our business was conducted by Adaptimmune Therapeutics plc and its consolidated subsidiaries, including Adaptimmune Limited. The historical consolidated financial statements of Adaptimmune Limited and consolidated subsidiary prior to the reorganization became those of Adaptimmune Therapeutics plc. For periods prior to the reorganization, the equity of Adaptimmune Therapeutics plc represents the historical equity of Adaptimmune Limited.
(3) The Company has identified that property and insurance costs relating to research and development facilities of $1,377,000 and $1,162,000 in the six months ended December 31, 2015 and the year ended June 30, 2015, respectively, were misclassified as general and administrative expenses in prior periods. These costs have been presented within research and development in the current period and the Company has reclassified prior period expenses to conform the presentation to the current period.
73
Table of Contents
Legal expenses for patent applications of $149,000, $303,000 and $171,000 in the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively, were misclassified as research and development expenditure in prior periods. These expenses have been presented within general administrative expenses in the current period and the Company has reclassified prior period expenses to conform the presentation to the current period.
The Company has assessed the materiality of the classification errors in accordance with the SEC’s guidance on assessing materiality, Staff Accounting Bulletin No. 99, Materiality, and determined that the errors are quantitatively and qualitatively not material.
The operating expenses for comparative periods as previously reported and as presented after the reclassification are as follows (in thousands):
|
|
|
Six months ended
December 31, 2015 |
|
Year ended
June 30, 2015 |
|
Year ended
June 30, 2014 |
|
|
|
|
As previously
reported |
|
After
reclassification |
|
As previously
reported |
|
After
reclassification |
|
As previously
reported |
|
After
reclassification |
|
|
Research and development |
|
$ |
24,244 |
|
$ |
25,472 |
|
$ |
23,278 |
|
$ |
24,137 |
|
$ |
9,746 |
|
$ |
9,575 |
|
|
General and administrative |
|
11,145 |
|
9,917 |
|
11,234 |
|
10,375 |
|
2,600 |
|
2,771 |
|
|
Total operating expenses |
|
$ |
35,389 |
|
$ |
35,389 |
|
$ |
34,512 |
|
$ |
34,512 |
|
$ |
12,346 |
|
$ |
12,346 |
|
74
Table of Contents
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion contains management’s discussion and analysis of our financial condition and results of operations and should be read together with “Selected Financial Data” and the historical consolidated financial statements and the notes thereto included in “Financial Statements and Supplementary Data”. This discussion contains forward-looking statements that reflect our plans, estimates and beliefs and involve numerous risks and uncertainties, including but not limited to those described in the “Risk Factors” section of this Annual Report. Actual results may differ materially from those contained in any forward-looking statements. You should carefully read “Special Note Regarding Forward-Looking Statements” and “Risk Factors.”
Overview
We are a clinical-stage biopharmaceutical company focused on novel cancer immunotherapy products based on its proprietary SPEAR T-cell platform. We have developed a comprehensive proprietary platform that enables us to identify cancer targets, find and genetically engineer TCR, and produce TCR therapeutic candidates for administration to patients. The Company engineers TCRs to increase their affinity to cancer specific peptides in order to destroy cancer cells in patients.
We have Phase 1/2 clinical trials ongoing with our NY-ESO and MAGE-A10 SPEAR T-cells and during 2016 opened two additional INDs for our AFP and MAGE A-4 SPEAR T-cells. Our NY-ESO SPEAR T-cell has shown promising initial results in clinical trials with a 50% response rate and 18-month median survival rate reported in synovial sarcoma (a solid tumor) and a 91% response rate at day 100 post autologous stem cell transplant in multiple myeloma. The NY-ESO SPEAR T-cell has shown a promising tolerability profile to date in all clinical trials. Our NY-ESO SPEAR T-cell therapy has breakthrough therapy designation in the United States and has also received orphan drug designation from the FDA and European Commission for the treatment of soft tissue sarcoma. The EMA has also granted PRIME regulatory access for the Company’s NY-ESO SPEAR T-cell therapy for the synovial sarcoma indication. We expect further clinical data during 2017.
In addition, we continue to use our SPEAR T-cell platform to identify further target peptides which provide additional coverage for any existing indications or which show high expression in specific cancers. We have identified over 30 intracellular target peptides and have 12 research programs evaluating these peptides.
The NY-ESO SPEAR T-cell program is subject to a collaboration and license agreement with GSK under which GSK has an option to obtain an exclusive worldwide license to the NY-ESO SPEAR T-cell program. In February 2016, the GSK Collaboration and License Agreement was expanded to accelerate the development of the NY-ESO SPEAR T-cells towards pivotal trials in synovial sarcoma, as well as the exploration of development of NY-ESO SPEAR T-cells in MRCLS. The amendment also provides the opportunity for up to eight combination studies using NY-ESO SPEAR T-cells. The Company achieved development milestones under the GSK Collaboration and License Agreement of $17.4 million in the year ended December 31, 2016.
Significant Events in the Three Months Ended December 31, 2016
· On October 18, 2016, the Company announced initiation of a Phase 1 triple tumor study using its wholly owned MAGE-A10 SPEAR T-cell therapy in patients with inoperable or metastatic urothelial cancer (transitional cell cancer of the bladder, ureter, or renal pelvis), melanoma, or squamous cell carcinoma of the head and neck.
· On October 27, 2016, the Company announced entry into a clinical trial collaboration agreement for the assessment of our NY-ESO SPEAR T-cell therapy in combination with Merck’s PD-1 inhibitor, KEYTRUDA® (pembrolizumab) in patients with multiple myeloma.
· On November 9, 2016, the Company announced that the FDA had removed the partial clinical hold on the planned study of its NY-ESO SPEAR in MRCLS. The MRCLS trial is now active at sites in the United States (the initiation of patient screening in this study was announced on December 5, 2016).
· On December 19, 2016, the Company announced entry into a Co-Development and Co-Commercialization Agreement with Bellicum in order to facilitate a staged collaboration to evaluate, develop and commercialize next generation T- cell therapies. Under the collaboration, we will evaluate Bellicum’s GoTCR technology (inducible MyD88/CD40 co-stimulation, or iMC) with our SPEAR T-cells for the potential to create enhanced T-cell therapeutics. Depending on results of the initial preclinical proof-of-concept phase, we may progress to a two-target co-development and co-commercialization phase.
Recent events since December 31, 2016
· On January 9, 2017, we announced that GSK had nominated a second target, PRAME (preferentially expressed antigen in melanoma), under the GSK Collaboration and License Agreement. Adaptimmune will be responsible for PRAME preclinical TCR development and delivery of the IND package to GSK.
75
Table of Contents
Financial operations overview
Revenue
In May 2014, the Company entered into the GSK Collaboration and License Agreement, for the development of, and option to obtain an exclusive license to, up to five SPEAR T-cell programs. The first of these programs is for the development of the Company’s NY-ESO SPEAR T-cells and the second of these programs is for the development of a PRAME SPEAR T-cell.
The revenue recognized to date relates to the upfront payment of $42.1 million received in June 2014 and non-substantive development milestones of $17.4 million, $14.4 million and $7.2 million achieved in the year ended December 31, 2016, six months ended December 31, 2015 and the year ended June 30, 2015, respectively.
Revenue relating to milestone payments is recognized using the proportional performance method systematically over the period in which the Company is delivering services under the GSK Collaboration and License Agreement, which is determined to be the period until GSK’s option to obtain licenses expires.
The Company is entitled to further non-substantive milestone payments based on the achievement of specified development milestones and royalties from GSK on all GSK sales of TCR therapeutic products licensed under the agreement. When, and if, GSK exercises its option to obtain an exclusive license to a target, an option exercise fee will be payable and the Company will be entitled to further development and commercialization milestone payments based on achievement of specified milestones by GSK.
Research and Development Expenses
Research and development expenses consist principally of the following:
· salaries for research and development staff and related expenses, including benefits;
· costs for production of preclinical compounds and drug substances by contract manufacturers;
· fees and other costs paid to contract research organizations in connection with additional preclinical testing and the performance of clinical trials;
· costs relating to facilities, materials and equipment used in R&D;
· costs of acquired or in-licensed R&D which does not have alternative future use;
· amortization and depreciation of property, plant and equipment and intangible assets used to develop our SPEAR T-cells; and
· share-based compensation expenses;
offset by:
· reimbursements from government grants; and
· reimbursable tax and expenditure credits from the U.K. government.
Research and development expenditures are expensed as incurred.
Our research and development expenses may vary substantially from period to period based on the timing of our research and development activities, which depends upon the timing of initiation of clinical trials and the rate of enrollment of patients in clinical trials. The duration, costs, and timing of clinical trials and development of our SPEAR T-cells will depend on a variety of factors, including:
· the scope, rate of progress, and expense of our ongoing as well as any additional clinical trials and other research and development activities;
· uncertainties in clinical trial enrollment rates;
· future clinical trial results;
· significant and changing government regulation;
· the timing and receipt of any regulatory approvals; and
· supply and manufacture of lentiviral vector and SPEAR T-cells for clinical trials.
76
Table of Contents
For further detail please see Part II — Item 1A Risk Factors — Risks Related to the Development of our SPEAR T-cells.
A change in the outcome of any of these variables may significantly change the costs and timing associated with the development of that SPEAR T cell. For example, if the FDA, or another regulatory authority, requires us to conduct clinical trials beyond those that we currently anticipate will be required for regulatory approval, or if we experience significant delays in enrollment in any of our clinical trials, we could be required to expend significant additional financial resources and time on the completion of clinical development.
General and Administrative Expenses
Our general and administrative expenses consist principally of:
· salaries for employees other than research and development staff, including benefits;
· business development expenses, including travel expenses;
· professional fees for auditors, lawyers and other consulting expenses;
· cost of facilities, communication, and office expenses;
· information technology expenses;
· amortization and depreciation of property, plant and equipment and intangible assets not related to research and development activities; and
· share-based compensation expenses.
Other Income (Expense), net
Other income (expense), net primarily comprises foreign exchange gains (losses). We are exposed to foreign exchange rate risk because we currently operate in the United Kingdom and United States. Our revenue from our GSK Collaboration and License Agreement is denominated in pounds sterling and is generated by our U.K.-based subsidiary, which has a pounds sterling functional currency. As a result, these sales are subject to translation into U.S. Dollars when we consolidate our financial statements. Our expenses are generally denominated in the currency in which our operations are located, which are the United Kingdom and United States. However, our U.K.-based subsidiary incurs significant research and development costs in U.S. dollars and, to a lesser extent, Euros.
Our results of operations and cash flows will be subject to fluctuations due to changes in foreign currency exchange rates, which could harm our business in the future. We seek to minimize this exposure by maintaining currency cash balances at levels appropriate to meet foreseeable expenses in U.S. dollars and pounds sterling. To date, we have not used hedging contracts to manage exchange rate exposure, although we may do so in the future.
Income Taxes
We are subject to corporate taxation in the United Kingdom and the United States. Our income tax recognized represents the tax currently payable arising on taxable profits from our U.S. subsidiary, which is subject to federal corporation tax of 34%. The U.S. subsidiary has been granted an exemption from certain state and local taxes, which we anticipate being in place for the next several years.
The Company incurs losses in the United Kingdom. No deferred tax assets are recognized on our U.K. losses because there is currently no indication that we shall make sufficient taxable profits to utilize these tax losses. Unsurrendered tax losses can be carried forward to be offset against future taxable profits. There are accumulated tax loss carry forwards in the United Kingdom amounting to $86.0 million at December 31, 2016. These tax losses do not expire. However, draft legislation has been published for inclusion in Finance Bill 2017 that would, if enacted, restrict the use of carried forward tax losses from April 1, 2017, such that they would not be available for offset against more than 50% of taxable profits in any accounting period (subject to a £5 million annual allowance).
In the future, if we generate taxable income in the United Kingdom, we may benefit from the United Kingdom’s “patent box” regime, which would allow certain profits attributable to revenues from patented products to be taxed at a rate that over time will be reduced to 10%. As we have many different patents covering our products, future upfront fees, milestone fees, product revenues, and royalties may be taxed at this favorably low tax rate.
VAT is charged on all qualifying goods and services by VAT-registered businesses. An amount of 20% of the value of the goods or services is added to all sales invoices and is payable to the U.K. tax authorities. Similarly, VAT paid on purchase invoices paid by Adaptimmune Limited and Adaptimmune Therapeutics plc is reclaimable from the U.K. tax authorities.
77
Table of Contents
Results of Operations
We have transitioned to reporting our results on a calendar year basis, and as such we are reporting herein results for the year ended December 31, 2016, the six-month period ended December 31, 2015, and the years ended June 30, 2015 and 2014 together with the results for the comparative period. The comparative results for the year ended December 31, 2015 and the six-month period ended December 31, 2014, have been recast for comparative purposes and have been prepared on the same basis as the audited consolidated financial statements and reflect, in the opinion of management, all adjustments of a normal, recurring nature that are necessary for a fair presentation of that consolidated financial information.
Comparison of Year Ended December 31, 2016 and 2015
The following table summarizes the results of our operations for the years ended December 31, 2016 and 2015, together with the changes to those items (in thousands):
|
|
|
Year ended
December 31, |
|
|
|
|
|
|
|
|
2016 |
|
2015 |
|
Increase/decrease |
|
|
Revenue |
|
$ |
14,198 |
|
$ |
14,490 |
|
$ |
(292 |
) |
(2 |
)% |
|
Research and development expenses |
|
(63,789 |
) |
(40,457 |
) |
(23,332 |
) |
58 |
% |
|
General and administrative expenses |
|
(23,208 |
) |
(17,156 |
) |
(6,052 |
) |
35 |
% |
|
Total operating expenses |
|
(86,997 |
) |
(57,613 |
) |
(29,384 |
) |
51 |
% |
|
Operating loss |
|
(72,799 |
) |
(43,123 |
) |
(29,676 |
) |
69 |
% |
|
Interest income |
|
1,110 |
|
787 |
|
323 |
|
41 |
% |
|
Other income, net |
|
1,002 |
|
2,967 |
|
(1,965 |
) |
(66 |
)% |
|
Loss before income taxes |
|
(70,687 |
) |
(39,369 |
) |
(31,318 |
) |
80 |
% |
|
Income taxes |
|
(892 |
) |
(143 |
) |
(749 |
) |
528 |
% |
|
Loss for the period |
|
$ |
(71,579 |
) |
$ |
(39,512 |
) |
$ |
(32,067 |
) |
81 |
% |
Revenue
Revenue decreased by two percent from $14.5 million for the year ended December 31, 2015 to $14.2 million for the year ended December 31, 2016. Revenue represents the upfront milestone payment, which is recognized over the period the Company will deliver services to GSK, and non-substantive milestone payments, which are allocated to the relevant deliverable and recognized over the period the Company delivers services to GSK. Revenue will typically increase in periods when development milestones are achieved, due to the recognition of revenue for the proportion of the milestone relating to past performance. The Company achieved development milestones of $17.4 million and $14.4 million in the year ended December 31, 2016 and 2015, respectively. The estimate of the period over which the Company will deliver services under the GSK Collaboration and License Agreement was increased in June and December 2016 which resulted in a decrease in revenue amortization of $5,615,000 in the year ended December 31, 2016 compared to the revenue that would have been recognized based on previous estimates.
The changes in estimate will also result in a decrease in revenue amortization of $2,237,000 in the year ended December 31, 2017 and an increase in revenue amortization of $939,000, $900,000 and $6,053,000 in the years ended December 31, 2018, 2019 and 2020, respectively, compared to the revenue that would have been recognized based on previous estimates.
Although it is difficult to project the timing of achieving future development deliverables, we expect revenue for the year ended December 31, 2017 will be higher than the year ended December 31, 2016 due to the potential achievement of development milestones in the period.
Research and development expenses
Research and development expenses increased by 58% to $63.8 million for the year ended December 31, 2016 from $40.5 million for the year ended December 31, 2015.
Our research and development expenses are highly dependent on the phases of our research projects and therefore fluctuate from period to period.
The increase in our research and development expenses of $23.3 million for the year ended December 31, 2016 compared to the same period in 2015 was primarily due to the following:
· a $15.6 million increase in salaries, materials, equipment, depreciation of property, plant and equipment and other employee-related costs. The driver for these is an increase in the average number of employees engaged in research and development from 108 to 210;
· a $10.3 million increase in subcontracted expenditures, including clinical trial expenses, CRO costs, and manufacturing expenses driven by increased recruitment in our clinical trials; and
78
Table of Contents
· a $0.5 million increase in payments for in-process R&D;
partially offset by:
· a $0.9 million decrease in share-based compensation expense due to a decrease in share-based compensation expense for nonemployee share options, which are remeasured at each reporting date, of $2.9 million offset by an increase in share-based compensation expense for employees of $2.0 million; and
· a $2.2 million increase in reimbursements in the form of grants and R&D tax and expenditure credits from the U.K. government.
Our subcontracted costs for the year ended December 31, 2016 were $23.6 million, of which $17.6 million related to our NY-ESO SPEAR T-cells and the remaining $6.0 million related to other projects, including our MAGE-A10, MAGE-A4 and AFP SPEAR T-cells.
In the year ended December 31, 2017, we plan to increase the number of clinical trials we are running, both in new therapies (including our MAGE-A4 and AFP SPEAR T-cells), in existing therapies (our MAGE-A10 SPEAR T-cell) and as part of the GSK Collaboration and License Agreement for our NY-ESO SPEAR T-cells. We expect to increase the number of staff employed in our research and development departments in order to invest in our future pipeline of SPEAR T-cells, develop our platform and manage clinical trials. This will significantly increase the related salaries and share-based compensation expense, as well as require higher expenditures on facilities, materials and consumables.
The share-based compensation expense will fluctuate in future periods due to changes in the assumptions to the fair value calculation for nonemployee share options, which include the share price, interest rates, volatility and expected term. A five percent increase in the share price at December 31, 2016 would have increased the share-based compensation expense for the year ended December 31, 2016 by approximately $33,000.
General and administrative expenses
General and administrative expenses increased by 35% to $23.2 million for the year ended December 31, 2016 from $17.2 million in the same period in 2015.
The increase of $6.0 million was due to the following:
· a $3.8 million increase in personnel costs, primarily due to the addition of key management and other professionals to support our growth;
· a $0.4 million increase in property costs, primarily due to an increase in leased property; and
· a $1.9 million increase in other corporate costs, including costs incurred as a U.S. public company such as consulting, audit, tax legal and investor relations fees and expenses;
partially offset by:
· a $0.1 million decrease in share-based compensation expense.
We expect that our general and administrative expenses will continue to increase as the Company continues to expand.
Other income, net
Other income, net decreased by 66% to $1.0 million for the year ended December 31, 2016 from $3.0 million for the year ended December 31, 2015. Other income, net primarily relates to unrealized foreign exchange gains/losses on cash and cash equivalents, intercompany loans and short-term deposits held in U.S. dollars by the Company’s U.K. subsidiary.
Income taxes
Income taxes increased by 528% to $0.9 million for the year ended December 31, 2016 from $0.1 million for the year ended December 31, 2015. Income taxes arise in the U.S. and the increase in income taxes is due to an increase in the taxable profits in the U.S. as the Company expands its operations. The Company incurs losses in the United Kingdom.
79
Table of Contents
Comparison of Six Months Ended December 31, 2015 and 2014
The following table summarizes the results of our operations for the six months ended December 31, 2015 and 2014, together with the changes to those items (in thousands).
|
|
|
Six months ended December 31, |
|
Increase/ |
|
|
|
|
2015 |
|
2014 |
|
decrease |
|
|
Revenue |
|
$ |
8,979 |
|
$ |
4,360 |
|
$ |
4,619 |
|
106 |
% |
|
Research and development |
|
(25,472 |
) |
(9,152 |
) |
(16,320 |
) |
178 |
% |
|
General and administrative |
|
(9,917 |
) |
(3,136 |
) |
(6,781 |
) |
216 |
% |
|
Total operating expenses |
|
(35,389 |
) |
(12,288 |
) |
(23,101 |
) |
188 |
% |
|
Operating loss |
|
(26,410 |
) |
(7,928 |
) |
(18,482 |
) |
233 |
% |
|
Interest income |
|
489 |
|
206 |
|
283 |
|
137 |
% |
|
Other income, net |
|
2,866 |
|
2,222 |
|
644 |
|
29 |
% |
|
Loss before income taxes |
|
(23,055 |
) |
(5,500 |
) |
(17,555 |
) |
319 |
% |
|
Income taxes |
|
55 |
|
(46 |
) |
101 |
|
(220 |
)% |
|
Loss for the period |
|
$ |
(23,000 |
) |
$ |
(5,546 |
) |
$ |
(17,454 |
) |
315 |
% |
Revenue
Revenue increased from $4.4 million for the six months ended December 31, 2014 to $9.0 million for the six months ended December 31, 2015 due to an increase in the services performed in the period and the achievement of development deliverables. This increase was primarily due to the recognition of revenue relating to achievement of development milestones, which is being recognized over the period in which we are delivering services under the GSK Collaboration and License Agreement, partially offset by the impact of a change in the estimate during the six months ended December 31, 2015 of the period over which the Company is delivering services under the GSK Collaboration and License Agreement.
Research and development expenses
Research and development expenses increased by 178% to $25.5 million for the six months ended December 31, 2015 from $9.2 million for the six months ended December 31, 2014.
Our research and development expenses are highly dependent on the phases of our research projects and therefore fluctuate from period to period.
The increase in our research and development expenses of $16.3 million in the six months ended December 31, 2015 compared to the same period in 2014 was primarily due to:
· a $7.5 million increase in salaries, materials, equipment, depreciation of tangible fixed assets and other employee-related costs. The driver for these is an increase in the average number of employees engaged in research and development from 46 to 137;
· a $0.9 million increase in share-based compensation expenses;
· a $1.0 million increase in property expenses;
· a $2.5 million payment to Universal Cells for in-process R&D; and
· a $4.4 million increase in subcontracted expenditures, including clinical trial expenses, CRO costs, and manufacturing expenses driven by increased recruitment in our clinical trials.
As of December 31, 2015, we employed an average of 26 employees responsible for development of our TCR therapeutic candidate targeting NY-ESO. The remainder of our scientific employees are engaged in developing our future pipeline. We have not historically tracked the internal headcount of each research and development project.
Our subcontracted costs for the six months ended December 31, 2015 were $8.6 million, of which $5.3 million related to our TCR therapeutic candidate targeting NY-ESO and the remaining $3.3 million related to other projects, including our MAGE-A10 and AFP TCR therapeutic candidates.
80
Table of Contents
General and administrative expenses
General and administrative expenses increased by 216% to $9.9 million for the six months ended December 31, 2015 from $3.1 million in the same period in 2014.
The increase of $6.8 million was due to:
· $1.4 million of increased personnel costs, primarily due to the addition of key management and other professionals to support our growth;
· $1.9 million of increased share-based payment expenses; and
· $3.5 million of increased other corporate costs, including costs in relation to our Nasdaq listing, legal entity restructuring, consultants, additional audit costs and investor relations.
Interest income
Interest income increased to $0.5 million for the six months ended December 31, 2015 from $0.2 million for the six months ended December 31, 2014. Interest income has increased due an increase in cash and cash equivalents and short-term deposits.
Other income
Other income increased by 29% to $2.9 million for the six months ended December 31, 2015 from $2.2 million for the six months ended December 31, 2014 due to a foreign exchange gains on foreign currency balances.
Income taxes
Income taxes was a $55,000 benefit for the six months ended December 31, 2015 and a $46,000 expense for the six months ended December 31, 2014.
81
Table of Contents
Comparison of Years Ended June 30, 2015 and 2014
The following table summarizes the results of our operations for the years ended June 30, 2015 and 2014, together with the changes to those items (in thousands).
|
|
|
Year ended June 30, |
|
Increase/ |
|
|
|
|
2015 |
|
2014 |
|
decrease |
|
|
Revenue |
|
$ |
9,871 |
|
$ |
825 |
|
$ |
9,046 |
|
1096 |
% |
|
Research and development |
|
(24,137 |
) |
(9,575 |
) |
(14,562 |
) |
152 |
% |
|
General and administrative |
|
(10,375 |
) |
(2,771 |
) |
(7,604 |
) |
274 |
% |
|
Total operating expenses |
|
(34,512 |
) |
(12,346 |
) |
(22,166 |
) |
180 |
% |
|
Operating loss |
|
(24,641 |
) |
(11,521 |
) |
(13,120 |
) |
114 |
% |
|
Interest income |
|
504 |
|
— |
|
504 |
|
N/A |
|
|
Other income (expense), net |
|
2,323 |
|
(5 |
) |
2,328 |
|
NM |
|
|
Loss before income taxes |
|
(21,814 |
) |
(11,526 |
) |
(10,288 |
) |
89 |
% |
|
Income taxes |
|
(244 |
) |
(75 |
) |
(169 |
) |
225 |
% |
|
Loss for the period |
|
$ |
(22,058 |
) |
$ |
(11,601 |
) |
$ |
(10,457 |
) |
90 |
% |
NM = not meaningful
Revenue
Revenue increased from $0.8 million for the year ended June 30, 2014 to $9.9 million for the year ended June 30, 2015 due to a full year of recognition of revenue under the GSK Collaboration and License Agreement, which was entered into on May 30, 2014.
Research and development expenses
Research and development expenses increased by 152% to $24.1 million for the year ended June 30, 2015 from $9.6 million for the year ended June 30, 2014. Our research and development expenses are highly dependent on the phases of our research projects and therefore fluctuate from year to year.
The $14.6 million increase in our research and development expenses in the year ended June 30, 2015 from the same period in 2014 was primarily due to an increase in two key drivers of our expenses:
· the increase in the average number of employees engaged in research and development from an average of 27 to 63. These costs include salaries, facilities, materials, equipment, depreciation of tangible fixed assets, and expenses for share-based compensation; and
· an increase in subcontracted expenditures, including clinical trial expenses, CRO costs, and manufacturing expenses driven by increased recruitment in our clinical trials.
In the year ended June 30, 2015, we employed an average of 13 employees working in our clinical and development teams, primarily responsible for development of our TCR therapeutic candidates targeting NY-ESO and MAGE-A10. The remainder of our scientific employees are engaged in developing our future pipeline. We have not historically tracked the internal costs of each research and development project.
Our subcontracted costs for the year ended June 30, 2015 were $8.8 million, of which $5.0 million related to our TCR therapeutic candidate targeting NY-ESO and the remaining $3.8 million related to other projects, including our MAGE-A10 TCR therapeutic candidate.
General and administrative expenses
General and administrative expenses increased by 274% to $10.4 million for the year ended June 30, 2015 from $2.8 million in the same period in 2014. The increase of $7.6 million was due to:
· $2.7 million of increased personnel costs, primarily due to the addition of key management and other professionals to support our growth;
· $1.4 million of increased share-based payment expenses; and
· $3.5 million of increased other corporate costs, including costs in relation to our Nasdaq listing, legal entity restructuring, consultants, additional audit costs and investor relations.
82
Table of Contents
Interest income
Interest income was $0.5 million for the year ended June 30, 2015 compared to no interest income for the year ended June 30, 2014. Interest income consisted of bank interest on cash balances and short-term deposits and has increased due to an increase in cash balances.
Other income (expense), net
Other income (expense), net increased to income of $2.3 million for the year ended June 30, 2015 compared to an expense of $5,000 for the year ended June 30, 2014. Other income (expense) primarily consisted of foreign exchange gains and losses on foreign currency transactions.
Income taxes
Income taxes increased 225% to $244,000 for the year ended June 30, 2015 from $75,000 in the year ended 30, June 2014. Income taxes arises on taxable income arising in the U.S. tax jurisdiction.
83
Table of Contents
Liquidity and Capital Resources
Sources of Funds
Since our inception, we have incurred significant net losses and negative cash flows from operations. We financed our operations primarily through an initial public offering, placements of equity securities, cash receipts under our GSK Collaboration and License Agreement, government grants and research and development tax and expenditure credits. From inception through to December 31, 2016, we have raised:
· $307.3 million, net of issue costs, through the issuance of shares, of which $176.0 million was raised through our initial public offering in May 2015;
· $79.9 million upfront fees and milestones under our GSK Collaboration and License Agreement;
· $2.6 million of income in the form of government grants from the United Kingdom; and
· $7.2 million in the form of U.K. research and development tax credits and receipts from the U.K. RDEC Scheme.
The Company uses a non-GAAP measure, Total Liquidity Position, which is defined as cash and cash equivalents plus short-term deposits, to evaluate the funds available to the Company in the near-term. A description of Total Liquidity Position and reconciliation to the most directly comparable U.S. GAAP measure are provided below under “Non-GAAP measures”.
As of December 31, 2016, we had cash and cash equivalents of $158.8 million, in addition to short-term deposits of $22.7 million. Our Total Liquidity Position as of December 31, 2016 was $181.5 million. We believe that our Total Liquidity Position as of December 31, 2016 will be sufficient to fund our operations, including currently anticipated research and development activities and planned capital spending, for at least the next twelve months.
Cash Flows
The following table summarizes the results of our cash flows for the year ended December 31, 2016 and December 31, 2015, six months ended December 31, 2015 and 2014 and the years ended June 30, 2015 and 2014 (in thousands).
|
|
|
Year ended
December 31, |
|
Six months ended
December 31, |
|
Year ended
June 30, |
|
|
|
|
2016 |
|
2015 |
|
2015 |
|
2014 |
|
2015 |
|
2014 |
|
|
Net cash (used in)/provided by operating activities |
|
(48,168 |
) |
(31,609 |
) |
(18,062 |
) |
(16,123 |
) |
(29,666 |
) |
36,835 |
|
|
Net cash provided by / (used in) investing activities |
|
17,755 |
|
(41,427 |
) |
(9,838 |
) |
(27,248 |
) |
(58,837 |
) |
(1,366 |
) |
|
Net cash provided by financing activities |
|
17 |
|
175,989 |
|
— |
|
98,872 |
|
274,861 |
|
14,714 |
|
|
Cash, cash equivalents and restricted cash |
|
162,796 |
|
198,771 |
|
198,771 |
|
101,664 |
|
229,046 |
|
51,179 |
|
Operating Activities
Year ended December 31, 2016 compared to December 31, 2015
Net cash used in operating activities increased by $16.6 million to $48.2 million for the year ended December 31, 2016 from $31.6 million for the year ended December 31, 2015. Net cash used in operating activities is significantly impacted by the timing of milestone payments received from GSK under the GSK Collaboration and License Agreement. In the year ended December 31, 2016, we received $19.8 million of milestone payments from GSK compared to $10.8 million in the year ended December 31, 2015. After taking into account the GSK milestone payments, the increase in cash used in operations of $25.6 million was primarily the result of an increase in research and development costs due to the ongoing advancement of our preclinical programs and clinical trials and an increase in general and administrative expenses.
Six months ended December 31, 2015 compared to December 31, 2014
Net cash used in operating activities increased by $2.0 million to $18.1 million for the six months ended December 31, 2015 from $16.1 million for the six months ended December 31, 2014. Net cash used in operating activities is significantly impacted by the timing of milestone payments received from GSK under the GSK Collaboration and License Agreement. In the six months ended December 31, 2015, we received $10.7 million of milestone payments from GSK compared to $7.2 million in the six months ended December 31, 2014 and in the six months ended December 31, 2014, we made a VAT payment of $8.4 million relating to a GSK milestone payment received in June 2014. After taking into account the GSK milestone payments, the remaining increase in cash used in operations of $13.9 million was primarily the result of an increase in research and development costs due to the ongoing advancement of our preclinical programs and clinical trials and an increase in general and administrative expenses.
84
Table of Contents
Year ended June 30, 2015 compared to June 30, 2014
Operating cash flows operating activities decreased by $66.5 million to net cash used in operating activities of $29.7 million for the year ended June 30, 2015 from net cash provided by operating activities of $36.8 million for the year ended June 30, 2014. In the year ended June 30, 2015, the Company received $10.7 million of milestone payments from GSK and paid $8.4 million of VAT associated with the milestone payments received in the prior period compared to receiving $42.1 million of milestone payments and $8.4 million of associated VAT in the year ended June 30, 2014. After taking into account the GSK milestone payments, the remaining increase in cash used in operations of $18.3 million was primarily driven by an increase in research and development costs due to the ongoing advancement of our preclinical programs and clinical trials and an increase in general and administrative expenses.
Components of cash flows from operating activities
Net cash used in operating activities of $48.2 million for the year ended December 31, 2016 comprised a net loss of $71.6 million offset by noncash items of $10.9 million and a net cash inflow of $12.5 million from changes in operating assets and liabilities. The noncash items consisted primarily depreciation expense on plant and equipment of $3.1 million and equity-settled share-based compensation expense of $8.8 million, partially offset by unrealized foreign exchange gains of $1.3 million.
Net cash used in operating activities of $18.1 million for the six months ended December 31, 2015 comprised a net loss of $23.0 million offset by noncash items of $1.9 million and a net cash inflow of $3.0 million from changes in operating assets and liabilities. The noncash items consisted primarily depreciation expense on plant and equipment of $1.2 million and equity-settled share-based compensation expense of $3.6 million, partially offset by unrealized foreign exchange gains of $2.9 million.
Net cash used in operating activities of $29.7 million for the year ended June 30, 2015 comprises net loss of $22.1 million and a net cash outflow of $15.4 million from changes in operating assets and liabilities, partially offset by noncash items of $7.8 million. The noncash items consisted primarily of depreciation expense on plant and equipment of $0.7 million and equity-settled share-based compensation expense of $7.1 million.
Net cash provided by operating activities of $36.8 million for the year ended June 30, 2014 comprised a net loss of $11.6 million offset by noncash items of $0.5 million and a net cash inflow of $47.9 million from changes in operating assets and liabilities. The noncash items consisted primarily of depreciation expense on plant and equipment of $0.2 million and equity-settled share-based compensation expense of $0.3 million.
Investing Activities
Net cash used in investing activities was $17.8 million, $9.8 million, $58.8 million and $1.4 million for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively. These amounts included purchases of property and equipment of $11.5 million, $9.6 million, $5.1 million and $1.4 million for the year ended December 31, 2016, the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively, and acquisition of intangibles of $1.3 million and $0.2 million for the year ended December 31, 2016 and the six months ended December 31, 2015. The purchases of property, plant and equipment for the year ended December 31, 2016 and the six months ended December 31, 2015 related predominantly to the expansion of our laboratory facilities in the United Kingdom and the United States.
The net cash used in investing activities in the year ended December 31, 2016, the six months ended December 31, 2015 and the year ended June 30, 2015 also included the investment in short-term cash deposits with maturities greater than three months but less than 12 months of $42.8 million, $16.6 million and $53.9 million, respectively, offset by cash inflows from maturity of short-term deposits of $73.4 million and $16.6 million in the year ended December 31, 2016 and the six months ended December 31, 2015.
Financing Activities
Net cash from financing activities was $17,000, $0, $274.9 million and $14.7 million for year ended December 31, 2016, six months ended December 31, 2015 and years ended June 30, 2015 and 2014, respectively.
Net cash from financing activities for the year ended December 31, 2016 consisted of proceeds from exercise of share options of $17,000.
Net cash from financing activities for the year ended June 30, 2015 consisted of proceeds from issuing Series A preferred shares of $98.9 million, net of issuance costs of $4.9 million, and proceeds from issuing 67,500,000 ordinary shares of $176.0 million, after the deduction of fees of $13.4 million. The preferred shares were automatically converted to ordinary shares on a 1:1 basis immediately prior to the admission to trading of our ADSs on NASDAQ.
85
Table of Contents
Net cash from financing activities for the year ended June 30, 2014 consisted of proceeds of $15.8 million from issuing ordinary shares and cash received upon exercise of share options of $0.2 million offset by a repayment of an overdraft facility of $1.3 million.
Non-GAAP Measures
Total Liquidity Position (a non-GAAP financial measure)
Total Liquidity Position (a non-GAAP financial measure) is defined as cash and cash equivalents plus short-term deposits. Each of these components appears in the consolidated balance sheet. The U.S. GAAP financial measures most directly comparable to Total Liquidity Position are cash and cash equivalents and short-term deposits as reported in the consolidated financial statements (in thousands).
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
|
Cash and cash equivalents |
|
$ |
158,779 |
|
$ |
194,263 |
|
|
Short-term deposits |
|
22,694 |
|
54,620 |
|
|
Total Liquidity Position |
|
$ |
181,473 |
|
$ |
248,883 |
|
The Company believes that the presentation of Total Liquidity Position provides useful information to investors because management reviews Total Liquidity Position as part of its management of overall liquidity, financial flexibility, capital structure and leverage.
Off-Balance Sheet Arrangements
We did not have during the periods presented, and we do not currently have, any off-balance sheet arrangements, as defined in the rules and regulations of the SEC other than operating leases as described in Note 14 of the consolidated financial statements included in Item 15 of this Annual Report.
Contractual Obligations
The following table summarizes our contractual commitments and obligations as of December 31, 2016 (in thousands):
|
|
|
Payments due by period |
|
|
|
|
Total |
|
Less than
1 year |
|
1 - 3 years |
|
3 - 5 years |
|
More than
5 years |
|
|
Operating lease obligations(1) |
|
$ |
32,586 |
|
$ |
2,112 |
|
$ |
6,116 |
|
$ |
6,375 |
|
$ |
17,983 |
|
|
Purchase obligations(2) |
|
67,215 |
|
40,382 |
|
18,468 |
|
6,796 |
|
1,569 |
|
|
Total contractual cash obligations |
|
$ |
99,801 |
|
$ |
42,494 |
|
$ |
24,584 |
|
$ |
13,171 |
|
$ |
19,552 |
|
(1) As of December 31, 2016, operating lease obligations primarily consists of minimum lease payments under non-cancellable leases for laboratory and office property in Oxfordshire, U.K. and Philadelphia, U.S.
(2) Purchase obligations include signed orders for capital equipment, clinical materials, clinical trial expenses and contract manufacturing, which have been committed but not yet received, committed funding under the MD Anderson strategic alliance and costs relating to the expansion of our laboratory and office space in Oxfordshire, U.K. and Philadelphia, U.S. The timing of the payments for clinical materials, clinical trial expenses and contract manufacturing may vary depending on the rate of progress of development and clinical trial enrollment rates.
Operating lease obligations
In July 2015, the Company entered into a long-term lease agreement, with an early termination option at 123 months, for offices and research facilities in Philadelphia, U.S. In October 2016, the lease commenced upon completion of construction. The related lease commitments are included in the table above.
In September 2015, the Company entered into an agreement for a 25-year lease, with early termination options, for a research and development facility in Oxfordshire, United Kingdom. In October 2016, the Company entered into the lease for that facility following the completion of construction. The related lease commitments are included in the table above.
Purchase obligations
On September 26, 2016, the Company announced that it had entered into a multi-year strategic alliance with MD Anderson designed to expedite the development of T-cell therapies for multiple types of cancer. The Company and MD Anderson will collaborate in a number of studies including clinical and preclinical development of Adaptimmune’s SPEAR T-cell therapies targeting NY-ESO, MAGE-A10 and future clinical stage first and second generation SPEAR T-cell therapies such as MAGE-A4 across a number of cancers, including bladder, lung, ovarian, head and neck, melanoma, synovial sarcoma, esophageal and gastric cancers. Under the terms of the alliance agreement, Adaptimmune has committed funding of at least US $19,644,000 to fund studies under the alliance agreement. Payment of this funding is contingent on mutual agreement to study orders, in order for any study to be included under the alliance, and the performance of set milestones by MD Anderson. The Company will make payments to MD Anderson as
86
Table of Contents
certain milestones are achieved. The timing and amount of future payments is uncertain. These milestones are included within ‘Purchase obligations’ above.
On June 16, 2016, we entered into a supply agreement with ThermoFisher for the supply of the Dynabeads® CD3/CD28 technology. The Dynabeads® CD3/CD28 technology is designed to isolate, activate and expand human T-cells, and is being used in the manufacturing of our affinity enhanced T-cell therapies. The supply agreement runs until December 31, 2025. Under the supply agreement we are required to purchase our requirements for CD3/CD28 magnetic bead product exclusively from ThermoFisher for a period of 5 years and there are also minimum purchasing obligations (which have been included in the purchase obligations above). ThermoFisher has the right to terminate the supply agreement for material breach or insolvency.
Other obligations
On November 25, 2015, the Company entered into a Research Collaboration and License Agreement relating to gene editing and HLA-engineering technology with Universal Cells. The Company paid an upfront license fee of $2.5 million to Universal Cells. A milestone payment of $3.0 million was made in February 2016 and the Company will make further payments of up to $44 million if certain development and product milestones are achieved. Universal Cells would also receive a profit-share payment for the first product, and royalties on sales of other products utilizing its technology. Future payments are not reflected in the table above because the timing of the payments is uncertain.
In 2012, we entered into a series of license and sub-license agreements with Life Technologies Corporation, part of ThermoFisher that provide the Company with a field-based exclusive license under certain intellectual property rights owned or controlled by ThermoFisher. The Company paid upfront license fees of $1.0 million relating to the license and sublicense agreements and has an obligation to pay minimum annual royalties (in the tens of thousands of U.S. dollars prior to licensed product approval and thereafter at a level of 50% of running royalties in the previous year), milestone payments and a low single-digit running royalty payable on the net selling price of each licensed product. Future payments are not reflected in the table above because the timing and amount of the payments are uncertain.
Critical Accounting Policies and Significant Judgments and Estimates
We have prepared our consolidated financial statements in accordance with U.S. GAAP. Our preparation of these consolidated financial statements requires us to make estimates, assumptions and judgments that affect the reported amounts of assets, liabilities, expenses and related disclosures at the date of the consolidated financial statements, as well as revenue and expenses during the reporting periods. We evaluate our estimates and judgments on an ongoing basis. We base our estimates on historical experience and on various other factors that we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results could therefore differ materially from these estimates under different assumptions or conditions.
While our significant accounting policies are described in more detail in Note 2 to our consolidated financial statements, we believe the following accounting policies to be critical to the judgments and estimates used in the preparation of our financial statements.
Revenue Recognition
Revenue is recognized when earned and realized or realizable, which is generally when persuasive evidence of an arrangement exists, delivery has occurred or services have been rendered, the seller’s price to the buyer is fixed or determinable, and collectability is reasonably assured. Where applicable, all revenues are stated net of value added and similar taxes.
The Company’s revenue currently arises from the GSK Collaboration and License Agreement entered into in May 2014 and amended in February 2016, which requires the Company to provide multiple deliverables to GSK. The Company recognizes revenue for arrangements with multiple deliverables by identifying the separable deliverables within the arrangement, whereby a deliverable is considered separable if it has value to the customer on a standalone basis. Contingent deliverables, such as the right to nominate further development targets, which represent a substantive option (i.e. the customer is not required or compelled to purchase the optional products or services) and not priced at a significant and incremental discount are not considered to be a deliverable at inception of the arrangement.
The non-contingent arrangement consideration is allocated between the separate deliverables using the relative selling price. The relative selling price is determined using vendor-specific objective evidence (“VSOE”), if available, third party evidence if VSOE is not available, or a best estimate of the standalone selling price if neither VSOE nor third party evidence is available. The best estimate of the selling price is estimated after considering all reasonably available information, including market data and conditions, entity-specific factors such as the cost structure of the deliverable, internal profit and pricing objectives and the stage of development, if appropriate. Revenue allocated to each deliverable is recognized as it is delivered. Where delivery occurs over time, revenue is systematically recognized over the period which the Company will be providing services.
87
Table of Contents
Amounts received prior to satisfying the revenue recognition criteria are recorded as deferred revenue in the Company’s consolidated balance sheet. Amounts expected to be recognized as revenue within the 12 months following the balance sheet date are classified as deferred revenue in current liabilities. Amounts not expected to be recognized as revenue within the 12 months following the balance sheet date are classified as deferred revenue, non-current.
Milestone payments which are non-refundable, non-creditable and contingent on achieving clinical milestones are recognized as revenues either on achievement of such milestones if the milestones are considered substantive or over the period the Company has continuing performance obligations, if the milestones are not considered substantive. When determining if a milestone is substantive, the Company considers the following factors:
· The degree of certainty in achieving the milestone,
· The frequency of milestone payments,
· The Company’s efforts, which result in achievement of the milestone,
· The amount of the milestone payment relative to the other deliverables and payment terms, and
· Whether the milestone payment is related to future performance or deliverables.
When a performance obligation is being delivered over time, the revenue is recognized over the performance period. The revenue relating to the upfront fee and non-substantive development milestones payments received from GSK are being recognized systematically using the proportional performance method over the period in which the Company is delivering services under the GSK Collaboration and License Agreement, which is determined to be the period until GSK’s option to obtain licenses expires. The period until GSK’s option to obtain licenses expires will vary depending on the progress of the development and we regularly review and monitor the performance of the GSK Collaboration and License Agreement to determine this period. If circumstances arise that change the estimate, this may result in increases or decreases in estimated revenues for the period, which are reflected in the period in which the circumstances that give rise to the change in estimate become known to management. In June and December 2016, the estimate of the period over which the Company will deliver services under the GSK Collaboration and License Agreement was increased. These changes in estimate resulted in a decrease in revenue amortization of $5,615,000 in the year ended December 31, 2016, compared to the revenue that would have been recognized based on previous estimates. The changes in estimate will also result in a decrease in revenue amortization of $2,237,000 in the year ended December 31, 2017 and an increase in revenue amortization of $939,000, $900,000 and $6,053,000 in the years ended December 31, 2018, 2019 and 2020, respectively, compared to the revenue that would have been recognized based on previous estimates.
In prior periods, changes in estimate of the period over which the Company will deliver services under the GSK Collaboration and License Agreement have not resulted in a significant impact on revenue recognized, however a small change in estimate can have a significant impact on the revenue recognized. For example, a further three month increase or decrease in the period over which the Company will deliver services under the GSK Collaboration and License Agreement would have reduced or increased revenue amortization by approximately $1.2 million for the year ended December 31, 2016.
Clinical Trial Expenses
Expenses related to clinical trials are recognized as services are received. Nonrefundable advance payments for services are deferred and recognized in the statement of operations as the services are rendered. This determination is based on an estimate of the services received and there may be instances when the payments to vendors exceed the level of services provided resulting in a prepayment of the clinical expense. If the actual timing of the performance of services varies from our estimate, the accrual or prepaid expense is adjusted accordingly.
As part of the process of preparing our financial statements, we are required to estimate our accrued expenses. This process involves reviewing open contracts and purchase orders, communicating with our personnel to identify services that have been performed on our behalf, and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of the actual cost. The majority of our service providers invoice us monthly in arrears for services performed. We make estimates of our accrued expenses as of each balance sheet date in our financial statements based on facts and circumstances known to us at that time. We may confirm the accuracy of our estimates with the applicable service providers and make adjustments if necessary. Examples of estimated accrued research and development expenses include fees paid to: CROs in connection with clinical trials; operators of investigative sites in connection with clinical trials; vendors in connection with preclinical development activities; and vendors related to product manufacturing, development and distribution of clinical supplies.
We base our expenses related to clinical trials on our estimates of the services received and efforts expended pursuant to contracts with multiple CROs that conduct and manage clinical trials on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract, and may result in uneven payment flows. Payments under some of these contracts depend on factors such as the successful enrollment of subjects and the completion of clinical trial milestones. In accruing service fees, we estimate the time period over which services will be performed and the level of effort to be expended in each period.
88
Table of Contents
If the actual timing of the performance of services or the level of effort varies from our estimate, we adjust the accrual or prepaid amount accordingly.
There may be instances in which payments made to our vendors will exceed the level of services provided and result in a prepayment of the clinical expense. For example, the strategic alliance with MD Anderson involves milestone payments made in advance of the service being provided. In recognizing the expense, we estimate the cost by patient enrolled and recognize this over the period between initial dosing and estimated cessation of patient monitoring activities. The duration of the clinical trial is estimated based on internal historical data and projections. There is limited data available and our estimate of the duration of the clinical may vary as we obtain further data.
Although we do not expect our estimates of the amounts, status and timing of services performed to be materially different from the actual amounts, status and timing of services performed, if they do vary, we may report amounts that are too high or too low in any particular period. To date, there has been no material difference between our estimates and the amount actually incurred.
R&D Tax and Expenditure Credits
Research and development expenditure is presented net of reimbursements from reimbursable tax and expenditure credits from the U.K. government. As a company that carries out extensive research and development activities, we benefit from the U.K. research and development tax credit regime for small and medium sized companies (“SME R&D Tax Credit Scheme”), whereby our principal research subsidiary company, Adaptimmune Limited, is able to surrender the trading losses that arise from its research and development activities for a payable tax credit of up to approximately 33.4% of eligible research and development expenditures. Qualifying expenditures largely comprise employment costs for research staff, consumables and certain internal overhead costs incurred as part of research projects for which we do not receive income. Subcontracted research expenditures are eligible for a cash rebate of up to approximately 21.7%. A large proportion of costs in relation to our pipeline research, clinical trials management and manufacturing development activities, all of which are being carried out by Adaptimmune Limited, are eligible for inclusion within these tax credit cash rebate claims.
Expenditures incurred in conjunction with the GSK Collaboration and License Agreement are not qualifying expenditures under the SME R&D Tax Credit Scheme but certain of these expenditures can be reimbursed through the U.K. research and development expenditure credit (RDEC) scheme. Under the RDEC scheme tax relief is given at 11% of 130% of allowable R&D costs.
Reimbursable tax and expenditure credits are recognized when it is probable that the Company has complied with any attached conditions and will receive the reimbursement. Management is required to develop estimates at each reporting date on the amount of the reimbursable tax and expenditure credits, which includes an estimate of qualifying expenditure. The tax and expenditure credits are claimed from Her Majesty’s Revenue and Customs (“HMRC”) as part of the annual U.K. tax return. Although, we do not expect our estimates to be materially different from amounts claimed and subsequently reimbursed by HMRC, if our estimates of the qualifying expenditure differ from the amount claimed, we may report amounts that are too high or too low in any particular period. To date, there has been no material difference between our estimates and the amount actually reimbursed.
Income Taxes
Income taxes for the period comprise current and deferred tax. Income tax is recognized in the consolidated statement of operations except to the extent that it relates to items recognized directly in equity, in which case it is recognized in equity.
Current tax is the expected tax payable or receivable on the taxable income or loss for the period using tax rates enacted at the balance sheet date.
Deferred tax is accounted for using the asset and liability method that requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of temporary differences between the financial statement carrying amount and the tax bases of assets and liabilities at the applicable tax rates. At December 31, 2016, we have deferred tax assets of $19.8 million, offset by deferred tax liabilities of $2.2 million and a valuation allowance of $17.6 million.
A valuation allowance is provided when it is more-likely-than-not that some portion or all of the deferred tax assets will not be realized. Future realization of the tax benefit of a deferred tax asset depends on the existence of sufficient taxable income of the appropriate character (for example, ordinary income or capital gain) within the carryback, carryforward period available under the tax law. The Company considers the following possible sources of taxable income when assessing whether there is sufficient taxable income to realize a tax benefit for deductible temporary differences and carryforwards:
· future reversals of existing taxable temporary differences;
· future taxable income exclusive of reversing temporary differences and carryforwards;
89
Table of Contents
· taxable income in prior carryback year(s) if carryback is permitted under the tax law; and
· tax-planning strategies.
The Company considers both positive and negative evidence regarding realization of the deferred tax assets and the subjectivity of this evidence. This assessment includes estimating future taxable income, scheduling reversals of temporary differences, evaluating expectations of future profitability, determining refund potential in the event of net operating loss carrybacks, and evaluating potential tax-planning strategies.
The Company has generated losses in the United Kingdom since inception and is forecasted to generate tax losses for the next several years and therefore the deferred tax assets arising in the United Kingdom are only considered more-likely-than-not of being realized to the extent that reversing temporary taxable differences are available.
The U.S. subsidiary has generated taxable income since the fiscal year ended June 30, 2014 and is forecast to generate taxable income in future periods. In determining whether the deferred tax asset that is more-likely-than-not of being recognized, the Company has taken into account the short history of taxable profits, the forecast of future taxable income, including whether future originating temporary deductible differences are likely to be realized, and the reversal of temporary taxable deductions. Several of the temporary deductible differences reverse over a long time period, such as those relating to share-based compensation expense, which the Company forecasts are likely to reverse predominately in 2020 and 2021. The Company considers that forecasting taxable income beyond the next few years is very subjective due to the nature and extent of the development process subcontracted from the Company in the United Kingdom to the U.S. subsidiary. Less weight has been given to forecasts of taxable income beyond the next few years. The deferred tax asset arising in the United States is only considered more-likely-than-not of being realized to the extent that there are available reversing temporary taxable differences. The Company’s analysis is subject to estimates and judgments particularly relating to the timing of the reversal of temporary deductible differences for stock compensation expense and the availability of future taxable income beyond the next few years, which depend on the nature and extent of the subcontract development work performed by the U.S. subsidiary.
Income tax positions must meet a more-likely-than-not recognition threshold to be recognized. Income tax positions that previously failed to meet the more-likely-than-not threshold are recognized in the first subsequent financial reporting period in which that threshold is met. Previously recognized tax positions that no longer meet the more-likely-than-not threshold are derecognized in the first subsequent financial reporting period in which that threshold is no longer met. Recognized income tax positions are measured at the largest amount that is greater than 50% likely of being realized. We recognize potential accrued interest and penalties related to unrecognized tax benefits within the consolidated statement of operations as income tax expense.
Share-based Compensation
The Company awards certain employees options over the ordinary shares of the parent company. The cost of share-based awards issued to employees is measured at the grant-date fair value of the award and recognized as an expense over the requisite service period, for those awards that are ultimately expected to vest. The fair value of the options is determined using the Black-Scholes option-pricing model. Share options with graded-vesting schedules are recognized on a straight-line basis over the requisite service period for each separately vesting portion of the award.
The Company has awarded share options to nonemployees for consultancy services. These share options are measured at the fair value of the goods/services received or the fair value of the equity instrument issued, whichever is more reliably measured, at the then-current fair values at each reporting date until the share options have vested and recognized as an expense over the requisite service period.
Valuation of Share Options
The Black-Scholes option pricing model requires the input of assumptions, including share price volatility, the expected term of a share option, the risk free rate and the underlying share valuation. The assumption of the expected term of share options involves management judgment. We estimate that the expected life of our share options, which is the time from the grant date to the expected exercise date, is five years. The life of the options depends on the option expiration date, volatility of the underlying shares and vesting features. We do not have sufficient history to determine the expected life based on internal data and therefore the estimate is based on empirical data. Due to the Company’s lack of sufficient history as a publicly traded company, management’s estimate of expected volatility is based on the average volatilities of seven public companies with similar attributes to the Company.
90
Table of Contents
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Market risk arises from our exposure to fluctuation in interest rates and currency exchange rates. These risks are managed by maintaining an appropriate mix of cash deposits in various currencies, placed with a variety of financial institutions for varying periods according to expected liquidity requirements.
We are exposed to market risks in the ordinary course of our business, which are principally limited to interest rate fluctuations and foreign currency exchange rate fluctuations, particularly between pound sterling and U.S. dollar. These risks are managed by maintaining an appropriate mix of cash deposits in various currencies, placed with a variety of financial institutions for varying periods according to expected liquidity requirements.
Interest Rate Risk
As of December 31, 2016, we had cash and cash equivalents of $158.8 million and short-term deposits of $22.7 million. Our exposure to interest rate sensitivity is impacted by changes in the underlying U.K. and U.S. bank interest rates. Our surplus cash and cash equivalents are invested in interest-bearing savings and money market accounts from time to time. We have not entered into investments for trading or speculative purposes. Due to the conservative nature of our investment portfolio, which is predicated on capital preservation of investments with short-term maturities, we do not believe an immediate one percentage point change in interest rates would have a material effect on the fair market value of our portfolio, and therefore we do not expect our operating results or cash flows to be significantly affected by changes in market interest rates.
Currency Risk
We are exposed to foreign exchange rate risk because we currently operate in the United Kingdom and the United States. Our revenue from the GSK Collaboration and License Agreement is denominated in pounds sterling and is generated by our U.K-based subsidiary, which has a pounds sterling functional currency. As a result, these sales are subject to translation into U.S. Dollars when we consolidate our financial statements. Our expenses are generally denominated in the currency in which our operations are located, which are the United Kingdom and the United States. However, our U.K.-based subsidiary incurs significant research and development costs in U.S. dollars and, to a lesser extent, Euros.
The results of operations and cash flows will be subject to fluctuations due to changes in foreign currency exchange rates, which could harm our business in the future. The exchange rate as at December 31, 2016, the last business day of the reporting period, was £1.00 to $1.233. The exchange rate on February 28, 2016 was £1.00 to $1.243. We seek to minimize this exposure by maintaining currency cash balances at levels appropriate to meet foreseeable expenses in U.S. dollars and pounds sterling. To date, we have not used forward exchange contracts or other currency hedging products to manage our exchange rate exposure, although we may do so in the future.
Credit Risk
The Company held cash and cash equivalents of $158.8 million and short-term deposits of $22.7 million as of December 31, 2016. The cash and cash equivalents and short-term deposits are held with multiple banks and the Company monitors the credit rating of those banks.
There are no material trade receivables as of December 31, 2016. Trade receivables may arise in future periods in relation to the GSK Collaboration and License Agreement. The Company has been transacting with GSK since 2014, during which time no impairment losses have been recognized. There are no amounts which are past due as of December 31, 2016.
Commodity Price Risk
We are exposed to commodity price risk as a result of our operations. However, given the size of our operations, the costs of managing exposure to commodity price risk exceed any potential benefits. We will revisit the appropriateness of this policy should our operations change in size or nature. We have no exposure to equity securities price risk as we hold no listed or other equity investments.
91
Table of Contents
Item 8. Financial Statements and Supplementary Data
The information required by this item may be found beginning on page F-1 of this Annual Report on Form 10-K with the exception of the unaudited consolidated quarterly operations data, which is presented below. We have prepared the consolidated quarterly operations data on a consistent basis with the audited consolidated financial statements included elsewhere in this Annual Report on Form 10-K. In the opinion of management, the quarterly consolidated operations data reflects all necessary adjustments, consisting only of normal recurring adjustments, necessary for a fair presentation of these data. Historical results are not necessarily indicative of the results to be expected in future periods, and the results for a quarterly period are not necessarily indicative of the operating results for a full year. This information should be read in conjunction with the consolidated financial statements included elsewhere in this Annual Report Form 10-K.
Summarized unaudited quarterly data for 2016 and 2015 are as follows (in thousands, except per share data):
|
|
|
Three months ended |
|
|
|
|
March 31,
2015 |
|
June 30,
2015 |
|
September 30,
2015 |
|
December 31,
2015 |
|
|
Revenue |
|
$ |
2,728 |
|
$ |
2,783 |
|
$ |
4,948 |
|
$ |
4,031 |
|
|
Operating loss |
|
(5,607 |
) |
(11,107 |
) |
(8,308 |
) |
(18,101 |
) |
|
Net loss |
|
(1,945 |
) |
(14,568 |
) |
(6,242 |
) |
(16,757 |
) |
|
Net loss attributable to ordinary shareholders |
|
(8,379 |
) |
(16,797 |
) |
(6,242 |
) |
(16,757 |
) |
|
Net loss per ordinary share, basic and diluted |
|
$ |
(0.05 |
) |
$ |
(0.05 |
) |
$ |
(0.01 |
) |
$ |
(0.04 |
) |
|
Weighted average shares outstanding, basic and diluted |
|
181,370,100 |
|
316,559,989 |
|
424,711,900 |
|
424,711,900 |
|
|
|
|
Three months ended |
|
|
|
|
March 31,
2016 |
|
June 30,
2016 |
|
September 30,
2016 |
|
December 31,
2016 |
|
|
Revenue |
|
$ |
2,918 |
|
$ |
328 |
|
$ |
2,416 |
|
$ |
8,536 |
|
|
Operating loss |
|
(16,825 |
) |
(22,700 |
) |
(18,618 |
) |
(14,656 |
) |
|
Net loss |
|
(15,576 |
) |
(22,095 |
) |
(18,494 |
) |
(15,414 |
) |
|
Net loss attributable to ordinary shareholders |
|
(15,576 |
) |
(22,095 |
) |
(18,494 |
) |
(15,414 |
) |
|
Net loss per ordinary share, basic and diluted |
|
$ |
(0.04 |
) |
$ |
(0.05 |
) |
$ |
(0.04 |
) |
$ |
(0.04 |
) |
|
Weighted average shares outstanding, basic and diluted |
|
424,711,900 |
|
424,711,900 |
|
424,711,900 |
|
424,720,404 |
|
92
Table of Contents
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None
Item 9A. Controls and Procedures
Disclosure Controls and Procedures.
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, has evaluated the effectiveness of our disclosure controls and procedures (as defined in Exchange Act Rules 13a-15(e) and 15d-15(e)) as of the end of the period covered by this Annual Report. Based on such evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that our disclosure controls and procedures were effective to ensure that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms, and is accumulated and communicated to our management, including our Chief Executive and Chief Financial Officer, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure.
Management’s Annual Report on Internal Control over Financial Reporting.
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Securities Exchange Act Rule 13a-15(f). Under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting based on the framework in Internal Control—Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on our evaluation under the framework, our management concluded that our internal control over financial reporting was effective as of December 31, 2016.
Attestation Report of the Registered Public Accounting Firm.
This report does not include an attestation report of our registered public accounting firm as we are an emerging growth company.
Changes in Internal Control Over Financial Reporting.
There has been no change in our internal control over financial reporting (as defined in Rule 13a-15(f) under the Exchange Act) that occurred during the fourth quarter of 2016 that has materially affected, or is reasonably likely to materially affect, internal control over financial reporting.
Item 9B. Other Information
None
93
Table of Contents
PART III
Item 10. Directors, Executive Officers and Corporate Governance
The information required under this item is incorporated herein by reference to our definitive proxy statement pursuant to Regulation 14A, to be filed with the Commission not later than 120 days after the close of our fiscal year ended December 31, 2016.
Item 11. Executive Compensation
The information required under this item is incorporated herein by reference to our definitive proxy statement pursuant to Regulation 14A, to be filed with the Commission not later than 120 days after the close of our fiscal year ended December 31, 2016.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information required under this item is incorporated herein by reference to our definitive proxy statement pursuant to Regulation 14A, to be filed with the Commission not later than 120 days after the close of our fiscal year ended December 31, 2016.
Item 13. Certain Relationships and Related Transactions, and Director Independence
The information required under this item is incorporated herein by reference to our definitive proxy statement pursuant to Regulation 14A, to be filed with the Commission not later than 120 days after the close of our fiscal year ended December 31, 2016.
Item 14. Principal Accounting Fees and Services
The information required under this item is incorporated herein by reference to our definitive proxy statement pursuant to Regulation 14A, to be filed with the Commission not later than 120 days after the close of our fiscal year ended December 31, 2016.
94
Table of Contents
PART IV
Item 15. Exhibits, Financial Statement Schedules
(a) 1. Financial Statements
As part of this Annual Report on Form 10-K, the consolidated financial statements are listed in the accompanying index to financial statements on page F-1.
2. Financial Statement Schedules
All schedules have been omitted because they are not required, not applicable, not present in amounts sufficient to require submission of the schedule, or the required information is otherwise included.
3. Exhibit Index
The following is a list of exhibits filed as part of this Annual Report on Form 10-K or are incorporated herein by reference:
|
Exhibit
Number |
|
Description of Exhibit |
|
3.1* |
|
Articles of Association of Adaptimmune Therapeutics plc (incorporated by reference to Exhibit 3.1 to our Form 8-K filed with the SEC on June 16, 2016). |
|
|
|
|
|
10.1* |
|
Letter of Appointment, dated May 23, 2016 and effective June 23, 2016, between the Company and Barbara Duncan (incorporated by reference to Exhibit 99.1 to our Form 8-K filed with the SEC on June 23, 2016). |
|
|
|
|
|
10.2* |
|
Letter of Appointment, dated August 9, 2016 and effective August 11, 2016, between the Company and David M. Mott (incorporated by reference to Exhibit 10.1 to our Form 8-K filed with the SEC on August 12, 2016). |
|
|
|
|
|
10.3* |
|
Letter of Appointment, dated August 9, 2016 and effective August 11, 2016, between the Company and Lawrence M. Alleva (incorporated by reference to Exhibit 10.2 to our Form 8-K filed with the SEC on August 12, 2016). |
|
|
|
|
|
10.4* |
|
Letter of Appointment, dated August 9, 2016 and effective August 11, 2016, between the Company and Ali Behbahani (incorporated by reference to Exhibit 10.3 to our Form 8-K filed with the SEC on August 12, 2016). |
|
|
|
|
|
10.5* |
|
Letter of Appointment, dated August 9, 2016 and effective August 11, 2016, between the Company and Ian M. Laing (incorporated by reference to Exhibit 10.4 to our Form 8-K filed with the SEC on August 12, 2016). |
|
|
|
|
|
10.6* |
|
Letter of Appointment, dated August 9, 2016 and effective August 11 2016, between the Company and Elliott Sigal (incorporated by reference to Exhibit 10.5 to our Form 8-K filed with the SEC on August 12, 2016). |
|
|
|
|
|
10.7* |
|
Letter of Appointment, dated August 9, 2016 and effective August 11, 2016, between the Company and Peter Thompson (incorporated by reference to Exhibit 10.6 to our Form 8-K filed with the SEC on August 12, 2016). |
|
|
|
|
|
10.8* |
|
Letter of Appointment, dated October 26, 2016 and effective November 1, 2016, between the Company and Giles Kerr (incorporated by reference to Exhibit 10.7 to our Form 10-Q filed with the SEC on November 10, 2016). |
|
|
|
|
|
10.9* |
|
Letter of Appointment, dated November 7, 2016 and effective November 14, 2016, between the Company and Tal Zaks (incorporated by reference to Exhibit 10.8 to our Form 10-Q filed with the SEC on November 10, 2016). |
|
|
|
|
|
10.10* |
|
First Amendment to Employment Agreement, dated September 6, 2016 and effective April 6, 2015, between Adaptimmune LLC and Adrian Rawcliffe (incorporated by reference to Exhibit 10.9 to our Form 10-Q filed with the SEC on November 10, 2016). |
|
|
|
|
|
10.11*†† |
|
Services Agreement, dated September 13, 2016, by and between Adaptimmune Limited and PCT, LLC (incorporated by reference to Exhibit 10.10 to our Form 10-Q filed with the SEC on November 10, 2016). |
|
|
|
|
|
10.12*†† |
|
Strategic Alliance Agreement, dated September 23, 2016, by and between Adaptimmune LLC and The University Of Texas M.D. Anderson Cancer Center (incorporated by reference to Exhibit 10.11 to our Form 10-Q filed with the SEC on November 10, 2016). |
|
|
|
|
|
10.13* |
|
Lease, dated October 24, 2016, by and between MEPC Milton Park No. 1 Limited and MEPC Milton Park No. 2 Limited, Adaptimmune Limited and Adaptimmune Therapeutics plc relating to 60 Jubilee Avenue Milton Park (incorporated by reference to Exhibit 10.12 to our Form 10-Q filed with the SEC on November 10, 2016). |
|
|
|
|
|
10.14*†† |
|
Clinical Trial Collaboration and Supply Agreement, dated October 27, 2016, by and between Merck Sharp & Dohme B.V. and Adaptimmune Limited (incorporated by reference to Exhibit 10.13 to our Form 10-Q filed with the SEC on November 10, 2016). |
95
Table of Contents
|
10.15* |
|
Letter, dated September 12, 2016, and effective November 8, 2016, between the Company and Immunocore Limited recording mutual agreement to terminate target collaboration agreement with termination effective on March 1, 2017 (incorporated by reference to Exhibit 10.14 to our Form 10-Q filed with the SEC on November 10, 2016). |
|
|
|
|
|
10.16**†† |
|
Co-Development and Co-Commercialisation Agreement, dated December 16, 2016, by and between Bellicum Pharmaceuticals, Inc. and Adaptimmune Limited. |
|
|
|
|
|
10.17** |
|
Service Agreement, dated March 10, 2017, and effective March 10, 2017, between Adaptimmune Therapeutics plc and James Noble. |
|
|
|
|
|
10.18** |
|
Employment Agreement, dated March 10, 2017, and effective March 10, 2017, between Adaptimmune LLC and Rafael Amado. |
|
|
|
|
|
10.19** |
|
Employment Agreement, dated March 10, 2017, and effective March 10, 2017, between Adaptimmune LLC and Gwendolyn Binder-Scholl. |
|
|
|
|
|
10.20** |
|
Employment Agreement, dated March 10, 2017, and effective March 10, 2017, between Adaptimmune LLC and Adrian Rawcliffe. |
|
|
|
|
|
10.21** |
|
Executive Severance policy of Adaptimmune Therapeutics plc, dated March 10, 2017, and effective March 10, 2017. |
|
|
|
|
|
10.22* |
|
Adaptimmune Limited Share Option Scheme (Incorporating Management Incentive Options), dated May 30, 2008, as amended January 13, 2016 (incorporated by reference to Exhibit 4.28 to our Transition Report on Form 20-F (file no. 001-37368). |
|
|
|
|
|
10.23* |
|
Adaptimmune Limited 2014 Share Option Scheme (Incorporating Enterprise Management Incentive Options), dated April 11, 2014, as amended January 13, 2016 (incorporated by reference to Exhibit 4.29 to our Transition Report on Form 20-F (file no. 001-37368). |
|
|
|
|
|
10.24* |
|
Adaptimmune Limited Company Share Option Plan, dated December 16, 2014, as amended January 13, 2016 (incorporated by reference to Exhibit 4.30 to our Transition Report on Form 20-F (file no. 001-37368). |
|
|
|
|
|
10.25* |
|
Adaptimmune Therapeutics plc 2015 Share Option Scheme, dated March 16, 2015, as amended April 15, 2015, as further amended January 13, 2016 (incorporated by reference to Exhibit 4.31 to our Transition Report on Form 20-F (file no. 001-37368). |
|
|
|
|
|
10.26* |
|
Adaptimmune Therapeutics plc Company Share Option Plan, dated March 16, 2015, as amended April 15, 2015, as further amended January 13, 2016 (incorporated by reference to Exhibit 4.32 to our Transition Report on Form 20-F (file no. 001-37368). |
|
|
|
|
|
10.27* |
|
Adaptimmune Therapeutics plc 2016 Employee Share Option Scheme, dated January 14, 2016 (incorporated by reference to Exhibit 4.33 to our Transition Report on Form 20-F (file no. 001-37368). |
|
|
|
|
|
21.1* |
|
List of Subsidiaries (incorporated by reference to Exhibit 21.1 to our Registration Statement on Form F-1 (file no: 333-203267)). |
|
|
|
|
|
23.1** |
|
Consent of KPMG LLP |
|
|
|
|
|
31.1** |
|
Certificate of Chief Executive Officer pursuant to 17 CFR 240.13a-14(a). |
|
|
|
|
|
31.2** |
|
Certificate of Chief Financial Officer pursuant to 17 CFR 240.13a-14(a). |
|
|
|
|
|
32.1** |
|
Certificate of Chief Executive Officer pursuant to 17 CFR 240.13a-14(b) and 18 U.S.C.1350. |
|
|
|
|
|
32.2** |
|
Certificate of Chief Financial Officer pursuant to 17 CFR 240.13a-14(b) and 18 U.S.C.1350. |
|
|
|
|
|
101.INS** |
|
XBRL Instance Document. |
|
|
|
|
|
101.SCH** |
|
XBRL Taxonomy Extension Schema Document. |
|
|
|
|
|
101.CAL** |
|
XBRL Taxonomy Extension Calculation Linkbase Document. |
|
|
|
|
|
101.DEF** |
|
XBRL Taxonomy Extension Definition Linkbase Document. |
96
Table of Contents
|
101.LAB** |
|
XBRL Taxonomy Extension Label Linkbase Document. |
|
|
|
|
|
101.PRE** |
|
XBRL Taxonomy Extension Presentation Linkbase Document. |
* Previously filed.
** Filed herewith.
† Confidential treatment previously requested by the Company and granted as to portions of the exhibit. Confidential materials omitted and filed separately with the Securities and Exchange Commission.
†† Confidential treatment requested by the Company as to portions of the exhibit. Confidential materials omitted and filed separately with the Securities and Exchange Commission.
97
Table of Contents
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, hereunto duly authorized, in Oxfordshire, England, on March 13, 2017.
|
|
ADAPTIMMUNE THERAPEUTICS PLC |
|
|
|
|
|
|
|
|
|
|
By: |
/s/ James Noble |
|
|
|
Name: |
James Noble |
|
|
|
Title: |
Chief Executive Officer and Director |
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints James Noble and Adrian Rawcliffe, and each of them, as his or her true and lawful attorney-in-fact and agent, with full power of substitution and resubstitution, for him or her and in his or her name, place and stead, in any and all capacities, to sign any and all amendments to this Annual Report on Form 10-K, and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing requisite and necessary to be done in connection therewith, as fully to all intents and purposes as he or she might or could do in person, hereby ratifying and confirming all that said attorneys-in-fact and agents, or any of them or their or his substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed by the following persons on March 13, 2017, in the capacities indicated.
|
Signature |
|
Title |
|
Date |
|
|
|
|
|
|
|
/s/ James Noble |
|
Chief Executive Officer and Director |
|
March 13, 2017 |
|
James Noble |
|
(Principal Executive Officer) |
|
|
|
|
|
|
|
|
|
/s/ Adrian Rawcliffe |
|
Chief Financial Officer |
|
March 13, 2017 |
|
Adrian Rawcliffe |
|
(Principal Accounting and Financial
Officer) |
|
|
|
|
|
|
|
|
|
/s/ David M. Mott |
|
Chairman of the Board of Directors |
|
March 13, 2017 |
|
David M. Mott |
|
|
|
|
|
|
|
|
|
|
|
/s/ Lawrence M. Alleva |
|
Director |
|
March 13, 2017 |
|
Lawrence M. Alleva |
|
|
|
|
|
|
|
|
|
|
|
/s/ Ali Behbahani, MD |
|
Director |
|
March 13, 2017 |
|
Ali Behbahani, MD |
|
|
|
|
|
|
|
|
|
|
|
/s/ Barbara Duncan |
|
Director |
|
March 13, 2017 |
|
Barbara Duncan |
|
|
|
|
|
|
|
|
|
|
|
/s/ Giles Kerr |
|
Director |
|
March 13, 2017 |
|
Giles Kerr |
|
|
|
|
|
|
|
|
|
|
|
/s/ Elliott Sigal, MD, PhD |
|
Director |
|
March 13, 2017 |
|
Elliott Sigal, MD, PhD |
|
|
|
|
|
|
|
|
|
|
|
/s/ Peter Thompson, MD |
|
Director |
|
March 13, 2017 |
|
Peter Thompson, MD |
|
|
|
|
|
|
|
|
|
|
|
/s/ Tal Zaks, MD, PhD |
|
Director |
|
March 13, 2017 |
|
Tal Zaks, MD, PhD |
|
|
|
|
98
Table of Contents
|
Index to the Financial Statements: |
|
|
|
|
|
|
|
Report of Independent Registered Public Accounting Firm |
|
F-2 |
|
|
|
|
|
Consolidated Balance Sheets as of December 31, 2016 and 2015 |
|
F-3 |
|
|
|
|
|
Consolidated Statement of Operations for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014 |
|
F-4 |
|
|
|
|
|
Consolidated Statements of Comprehensive Loss for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014 |
|
F-5 |
|
|
|
|
|
Consolidated Statements of Changes in Equity for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014 |
|
F-6 |
|
|
|
|
|
Consolidated Statements of Cash Flows for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014 |
|
F-8 |
|
|
|
|
|
Notes to the Consolidated Financial Statements |
|
F-9 |
F-1
Table of Contents
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders Adaptimmune Therapeutics plc:
We have audited the accompanying consolidated balance sheets of Adaptimmune Therapeutics plc and subsidiaries as of December 31, 2016, December 31, 2015 and June 30, 2015, and the related consolidated statements of operations, comprehensive loss, changes in equity and cash flows for the year ended December 31, 2016, the six month period ended December 31, 2015 and the years ended June 30, 2015 and June 30, 2014. These consolidated financial statements are the responsibility of Adaptimmune Therapeutic plc’s management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Adaptimmune Therapeutics plc and subsidiaries as of December 31, 2016, December 31, 2015 and June 30, 2015, and the results of their operations and their cash flows for the year ended December 31, 2016, the six month period ended December 31, 2015 and the years ended June 30, 2015 and June 30, 2014 in conformity with U.S. generally accepted accounting principles.
|
/s/ KPMG LLP |
|
|
|
Reading, United Kingdom |
|
March 13, 2017 |
F-2
Table of Contents
ADAPTIMMUNE THERAPEUTICS PLC
CONSOLIDATED BALANCE SHEETS
(in thousands, except share data)
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
|
Assets |
|
|
|
|
|
|
|
|
Current assets |
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
158,779 |
|
$ |
194,263 |
|
$ |
229,046 |
|
|
Short-term deposits |
|
22,694 |
|
54,620 |
|
55,292 |
|
|
Accounts receivable, net of allowance for doubtful accounts of $-, $- and $- (including amounts due from related parties of $-, $2 and $3) |
|
1,480 |
|
744 |
|
4 |
|
|
Other current assets and prepaid expenses (including current portion of clinical materials) |
|
15,798 |
|
13,420 |
|
10,740 |
|
|
Total current assets |
|
198,751 |
|
263,047 |
|
295,082 |
|
|
|
|
|
|
|
|
|
|
|
Restricted cash |
|
4,017 |
|
4,508 |
|
— |
|
|
Clinical materials |
|
2,580 |
|
4,736 |
|
— |
|
|
Property, plant and equipment, net |
|
27,899 |
|
13,225 |
|
5,393 |
|
|
Intangibles, net |
|
1,268 |
|
305 |
|
178 |
|
|
Total assets |
|
$ |
234,515 |
|
$ |
285,821 |
|
$ |
300,653 |
|
|
|
|
|
|
|
|
|
|
|
Liabilities and stockholders’ equity |
|
|
|
|
|
|
|
|
Current liabilities |
|
|
|
|
|
|
|
|
Accounts payable (including amounts due to related parties of $326, $- and $143) |
|
$ |
11,350 |
|
$ |
7,884 |
|
$ |
1,982 |
|
|
Accrued expenses and other accrued liabilities (including amounts due to related parties of $39, $288 and $2) |
|
17,528 |
|
7,518 |
|
3,877 |
|
|
Deferred revenue |
|
11,392 |
|
12,487 |
|
20,906 |
|
|
Total current liabilities |
|
40,270 |
|
27,889 |
|
26,765 |
|
|
|
|
|
|
|
|
|
|
|
Deferred revenue, non-current |
|
24,962 |
|
22,939 |
|
14,885 |
|
|
Accrued expenses, non-current |
|
3,141 |
|
— |
|
— |
|
|
|
|
|
|
|
|
|
|
|
Total liabilities |
|
68,373 |
|
50,828 |
|
41,650 |
|
|
|
|
|
|
|
|
|
|
|
Contingencies and commitments — Note 8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stockholders’ equity |
|
|
|
|
|
|
|
|
Common stock - Ordinary shares par value £0.001, 574,711,900 authorized and 424,775,092 issued and outstanding (December 31, 2015 and June 30, 2015: 574,711,900 authorized and 424,711,900 issued and outstanding) |
|
683 |
|
682 |
|
682 |
|
|
Additional paid in capital |
|
341,200 |
|
332,363 |
|
328,795 |
|
|
Accumulated other comprehensive loss |
|
(14,249 |
) |
(8,139 |
) |
(3,561 |
) |
|
Accumulated deficit |
|
(161,492 |
) |
(89,913 |
) |
(66,913 |
) |
|
Total stockholders’ equity |
|
166,142 |
|
234,993 |
|
259,003 |
|
|
|
|
|
|
|
|
|
|
|
Total liabilities and stockholders’ equity |
|
$ |
234,515 |
|
$ |
285,821 |
|
$ |
300,653 |
|
See accompanying notes to consolidated financial statements.
F-3
Table of Contents
ADAPTIMMUNE THERAPEUTICS PLC
CONSOLIDATED STATEMENTS OF OPERATIONS
(in thousands, except share and per share data)
|
|
|
Year ended
December 31,
2016 |
|
Six months ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Revenue |
|
$ |
14,198 |
|
$ |
8,979 |
|
$ |
9,871 |
|
$ |
825 |
|
|
Operating expenses |
|
|
|
|
|
|
|
|
|
|
Research and development |
|
(63,789 |
) |
(25,472 |
) |
(24,137 |
) |
(9,575 |
) |
|
General and administrative |
|
(23,208 |
) |
(9,917 |
) |
(10,375 |
) |
(2,771 |
) |
|
Total operating expenses (including purchases from related parties, net of reimbursements, of $2,067, $1,609, $2,443 and $2,018) |
|
(86,997 |
) |
(35,389 |
) |
(34,512 |
) |
(12,346 |
) |
|
Operating loss |
|
(72,799 |
) |
(26,410 |
) |
(24,641 |
) |
(11,521 |
) |
|
Interest income |
|
1,110 |
|
489 |
|
504 |
|
— |
|
|
Other income (expense), net |
|
1,002 |
|
2,866 |
|
2,323 |
|
(5 |
) |
|
Loss before income taxes |
|
(70,687 |
) |
(23,055 |
) |
(21,814 |
) |
(11,526 |
) |
|
Income taxes |
|
(892 |
) |
55 |
|
(244 |
) |
(75 |
) |
|
Net loss |
|
(71,579 |
) |
(23,000 |
) |
(22,058 |
) |
(11,601 |
) |
|
|
|
|
|
|
|
|
|
|
|
|
Deemed dividend on convertible preferred shares |
|
— |
|
— |
|
(14,735 |
) |
— |
|
|
Net loss attributable to ordinary shareholders |
|
$ |
(71,579 |
) |
$ |
(23,000 |
) |
$ |
(36,793 |
) |
$ |
(11,601 |
) |
|
|
|
|
|
|
|
|
|
|
|
|
Net loss per ordinary share basic and diluted (Note 2) |
|
$ |
(0.17 |
) |
$ |
(0.05 |
) |
$ |
(0.17 |
) |
$ |
(0.08 |
) |
|
|
|
|
|
|
|
|
|
|
|
|
Weighted average shares outstanding, basic and diluted |
|
424,713,997 |
|
424,711,900 |
|
214,704,593 |
|
148,335,529 |
|
See accompanying notes to consolidated financial statements.
F-4
Table of Contents
ADAPTIMMUNE THERAPEUTICS PLC
CONSOLIDATED STATEMENTS OF COMPREHENSIVE LOSS
(in thousands)
|
|
|
Year ended
December 31,
2016 |
|
Six months ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(71,579 |
) |
$ |
(23,000 |
) |
$ |
(22,058 |
) |
$ |
(11,601 |
) |
|
Other comprehensive loss, net of tax |
|
|
|
|
|
|
|
|
|
|
Foreign currency translation adjustments |
|
(6,110 |
) |
(4,578 |
) |
(3,835 |
) |
377 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Total comprehensive loss for the period |
|
$ |
(77,689 |
) |
$ |
(27,578 |
) |
$ |
(25,893 |
) |
$ |
(11,224 |
) |
See accompanying notes to consolidated financial statements.
F-5
Table of Contents
ADAPTIMMUNE THERAPEUTICS PLC
CONSOLIDATED STATEMENTS OF CHANGES IN EQUITY
(in thousands, except share data)
|
|
|
Common
stock |
|
Common
stock |
|
Additional
paid in capital |
|
Accumulated
other
comprehensive
(loss) income |
|
Accumulated
deficit |
|
Total
stockholders’
equity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Balance at July 1, 2013 |
|
109,783,500 |
|
$ |
177 |
|
$ |
16,290 |
|
$ |
(103 |
) |
$ |
(18,519 |
) |
$ |
(2,155 |
) |
|
Issuance of common stock |
|
70,208,600 |
|
112 |
|
15,700 |
|
— |
|
— |
|
15,812 |
|
|
Issuance of common stock upon exercise of share options |
|
1,378,000 |
|
2 |
|
190 |
|
— |
|
— |
|
192 |
|
|
Other comprehensive income, net of tax |
|
— |
|
— |
|
— |
|
377 |
|
— |
|
377 |
|
|
Net loss |
|
— |
|
— |
|
— |
|
— |
|
(11,601 |
) |
(11,601 |
) |
|
Share-based compensation expense |
|
— |
|
— |
|
332 |
|
— |
|
— |
|
332 |
|
|
Balance at June 30, 2014 |
|
181,370,100 |
|
$ |
291 |
|
$ |
32,512 |
|
$ |
274 |
|
$ |
(30,120 |
) |
$ |
2,957 |
|
|
|
|
Common
stock |
|
Common
stock |
|
Preferred
shares |
|
Additional
paid in capital |
|
Accumulated
other
comprehensive
income (loss) |
|
Accumulated
deficit |
|
Total
stockholders’
equity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Balance at July 1, 2014 |
|
181,370,100 |
|
$ |
291 |
|
$ |
— |
|
$ |
32,512 |
|
$ |
274 |
|
$ |
(30,120 |
) |
$ |
2,957 |
|
|
Issuance of preferred shares |
|
— |
|
— |
|
98,872 |
|
— |
|
— |
|
— |
|
98,872 |
|
|
Beneficial conversion feature |
|
— |
|
— |
|
(102,126 |
) |
102,126 |
|
— |
|
— |
|
— |
|
|
Issuance of common stock upon initial public offering, net of issuance costs |
|
67,500,000 |
|
104 |
|
— |
|
175,885 |
|
— |
|
— |
|
175,989 |
|
|
Issuance of common stock upon conversion of preferred shares |
|
175,841,800 |
|
287 |
|
(11,481 |
) |
11,194 |
|
— |
|
— |
|
— |
|
|
Deemed dividends on preferred shares |
|
— |
|
— |
|
14,735 |
|
— |
|
— |
|
(14,735 |
) |
— |
|
|
Other comprehensive loss, net of tax |
|
— |
|
— |
|
— |
|
— |
|
(3,835 |
) |
— |
|
(3,835 |
) |
|
Net loss |
|
— |
|
— |
|
— |
|
— |
|
— |
|
(22,058 |
) |
(22,058 |
) |
|
Share-based compensation expense |
|
— |
|
— |
|
— |
|
7,078 |
|
— |
|
— |
|
7,078 |
|
|
Balance at June 30, 2015 |
|
424,711,900 |
|
$ |
682 |
|
$ |
— |
|
$ |
328,795 |
|
$ |
(3,561 |
) |
$ |
(66,913 |
) |
$ |
259,003 |
|
F-6
Table of Contents
ADAPTIMMUNE THERAPEUTICS PLC
CONSOLIDATED STATEMENTS OF CHANGES IN EQUITY (CONTINUED)
(in thousands, except share data)
|
|
|
Common stock |
|
Common stock |
|
Additional
paid in capital |
|
Accumulated
other
comprehensive
loss |
|
Accumulated
deficit |
|
Total
stockholders’
equity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Balance at July 1, 2015 |
|
424,711,900 |
|
$ |
682 |
|
$ |
328,795 |
|
$ |
(3,561 |
) |
$ |
(66,913 |
) |
$ |
259,003 |
|
|
Other comprehensive loss, net of tax |
|
— |
|
— |
|
— |
|
(4,578 |
) |
— |
|
(4,578 |
) |
|
Net loss |
|
— |
|
— |
|
— |
|
— |
|
(23,000 |
) |
(23,000 |
) |
|
Share-based compensation expense |
|
— |
|
— |
|
3,568 |
|
— |
|
— |
|
3,568 |
|
|
Balance at December 31, 2015 |
|
424,711,900 |
|
$ |
682 |
|
$ |
332,363 |
|
$ |
(8,139 |
) |
$ |
(89,913 |
) |
$ |
234,993 |
|
|
|
|
Common stock |
|
Common stock |
|
Additional
paid in capital |
|
Accumulated
other
comprehensive
loss |
|
Accumulated
deficit |
|
Total
stockholders’
equity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Balance at January 1, 2016 |
|
424,711,900 |
|
$ |
682 |
|
$ |
332,363 |
|
$ |
(8,139 |
) |
$ |
(89,913 |
) |
$ |
234,993 |
|
|
Issuance of shares upon exercise of stock options |
|
63,192 |
|
1 |
|
16 |
|
— |
|
— |
|
17 |
|
|
Other comprehensive loss, net of tax |
|
— |
|
— |
|
— |
|
(6,110 |
) |
— |
|
(6,110 |
) |
|
Net loss |
|
— |
|
— |
|
— |
|
— |
|
(71,579 |
) |
(71,579 |
) |
|
Share-based compensation expense |
|
— |
|
— |
|
8,821 |
|
— |
|
— |
|
8,821 |
|
|
Balance at December 31, 2016 |
|
424,775,092 |
|
$ |
683 |
|
$ |
341,200 |
|
$ |
(14,249 |
) |
$ |
(161,492 |
) |
$ |
166,142 |
|
See accompanying notes to consolidated financial statements.
F-7
Table of Contents
ADAPTIMMUNE THERAPEUTICS PLC
CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands)
|
|
|
Year ended
December 31,
2016 |
|
Six months ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
Cash flows from operating activities |
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(71,579 |
) |
$ |
(23,000 |
) |
$ |
(22,058 |
) |
$ |
(11,601 |
) |
|
Adjustments to reconcile net income to net cash (used in) provided by operating activities: |
|
|
|
|
|
|
|
|
|
|
Depreciation |
|
3,126 |
|
1,176 |
|
705 |
|
240 |
|
|
Amortization |
|
160 |
|
69 |
|
30 |
|
— |
|
|
Loss on disposal |
|
122 |
|
— |
|
— |
|
— |
|
|
Share-based compensation expense |
|
8,821 |
|
3,568 |
|
7,078 |
|
332 |
|
|
Unrealized foreign exchange (gains) losses |
|
(1,314 |
) |
(2,867 |
) |
13 |
|
— |
|
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
|
Increase in receivables and other operating assets |
|
(6,533 |
) |
(4,243 |
) |
(7,812 |
) |
(1,481 |
) |
|
Decrease (increase) in non-current operating assets |
|
2,221 |
|
(4,736 |
) |
— |
|
— |
|
|
Increase (decrease) in payables and deferred revenue |
|
16,808 |
|
11,971 |
|
(7,622 |
) |
49,345 |
|
|
Net cash (used in) provided by operating activities |
|
(48,168 |
) |
(18,062 |
) |
(29,666 |
) |
36,835 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash flows from investing activities |
|
|
|
|
|
|
|
|
|
|
Acquisition of property, plant and equipment |
|
(11,506 |
) |
(9,628 |
) |
(5,080 |
) |
(1,366 |
) |
|
Acquisition of intangibles |
|
(1,279 |
) |
(210 |
) |
— |
|
— |
|
|
Proceeds from sale of property, plant and equipment |
|
— |
|
— |
|
122 |
|
— |
|
|
Maturity of short-term deposits |
|
73,377 |
|
16,645 |
|
— |
|
— |
|
|
Investment in short-term deposits |
|
(42,837 |
) |
(16,645 |
) |
(53,879 |
) |
— |
|
|
Net cash provided by (used in) investing activities |
|
17,755 |
|
(9,838 |
) |
(58,837 |
) |
(1,366 |
) |
|
|
|
|
|
|
|
|
|
|
|
|
Cash flows from financing activities |
|
|
|
|
|
|
|
|
|
|
Proceeds from issuance of preferred shares, net of issuance costs of $4,949 |
|
— |
|
— |
|
98,872 |
|
— |
|
|
Proceeds from issuance of common stock upon initial public offering, net of issuance costs of $13,387 |
|
— |
|
— |
|
175,989 |
|
— |
|
|
Proceeds from issuance of common stock |
|
— |
|
— |
|
— |
|
15,812 |
|
|
Proceeds from exercise of stock options |
|
17 |
|
— |
|
— |
|
192 |
|
|
Bank overdraft repaid |
|
— |
|
— |
|
— |
|
(1,290 |
) |
|
Net cash provided by financing activities |
|
17 |
|
— |
|
274,861 |
|
14,714 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Effect of currency exchange rate changes on cash and cash equivalents |
|
(5,579 |
) |
(2,375 |
) |
(8,491 |
) |
996 |
|
|
Net (decrease) increase in cash, cash equivalents and restricted cash |
|
(35,975 |
) |
(30,275 |
) |
177,867 |
|
51,179 |
|
|
Cash, cash equivalents and restricted cash at start of period |
|
198,771 |
|
229,046 |
|
51,179 |
|
— |
|
|
Cash, cash equivalents and restricted cash at end of period |
|
$ |
162,796 |
|
$ |
198,771 |
|
$ |
229,046 |
|
$ |
51,179 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Supplemental cash flow information |
|
|
|
|
|
|
|
|
|
|
Interest received |
|
$ |
1,191 |
|
$ |
326 |
|
$ |
— |
|
$ |
— |
|
|
Income taxes paid |
|
34 |
|
95 |
|
280 |
|
— |
|
|
Deemed dividends |
|
— |
|
— |
|
14,735 |
|
— |
|
|
Investment in restricted cash |
|
— |
|
4,666 |
|
— |
|
— |
|
|
Allowance for tenant improvements |
|
2,607 |
|
— |
|
— |
|
— |
|
See accompanying notes to consolidated financial statements.
F-8
Table of Contents
ADAPTIMMUNE THERAPEUTICS PLC
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Note 1 - General
Adaptimmune Therapeutics plc is registered in England and Wales. Its registered office is 101 Park Drive, Milton Park, Abingdon, Oxfordshire, OX14 4RY, United Kingdom. Adaptimmune Therapeutics plc and its subsidiaries, Adaptimmune Limited and Adaptimmune LLC, (collectively “Adaptimmune” or the “Company”) is a clinical-stage biopharmaceutical company focused on novel cancer immunotherapy products based on its proprietary SPEAR (Specific Peptide Enhanced Affinity Receptor) T-cell platform. It has developed a comprehensive proprietary platform that enables it to identify cancer targets, find and genetically engineer T-cell receptors (“TCRs”), and produce TCR therapeutic candidates for administration to patients. The Company engineers TCRs to increase their affinity to cancer specific peptides in order to destroy cancer cells in patients.
The Company is subject to a number of risks similar to other biopharmaceutical companies in the early stage including, but not limited to, the need to obtain adequate additional funding, possible failure of preclinical programs or clinical trials, the need to obtain marketing approval for its SPEAR T-cells, competitors developing new technological innovations, the need to successfully commercialize and gain market acceptance of the Company’s SPEAR T-cells, the need to develop a suitable commercial manufacturing process and protection of proprietary technology. If the Company does not successfully commercialize any of its SPEAR T-cells, it will be unable to generate product revenue or achieve profitability. The Company had an accumulated deficit of $161.5 million as of December 31, 2016.
Note 2 - Summary of Significant Accounting Policies
(a) Basis of presentation
The consolidated financial statements of Adaptimmune Therapeutics plc and its subsidiaries and other financial information included in this Annual Report have been prepared in accordance with generally accepted accounting principles in the United States of America (“US GAAP”) and are presented in U.S. dollars. All significant intercompany accounts and transactions between the Company and its subsidiaries have been eliminated on consolidation.
The Company undertook a reorganization that was completed in April 2015 and is described in Note 9. As appropriate for a reorganization of entities under common control, the historical consolidated financial statements of Adaptimmune Limited and subsidiary prior to the reorganization became those of Adaptimmune Therapeutics plc.
On February 23, 2015 the Company undertook a one-for-100 share exchange. All share and per share information presented gives effect to the reorganization by dividing the loss for the period by the weighted average number of shares outstanding of Adaptimmune Therapeutics plc as if the one-for-100 share exchange had been in effect throughout the period. The nominal value of the share capital has been increased to reflect the nominal share capital after the one-for-100 share exchange.
(b) Use of estimates in financial statements
The preparation of financial statements, in conformity with U.S. GAAP and SEC regulations, requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities, disclosure of contingent assets and liabilities at the date of the consolidated financial statements and reported amounts of revenues and expenses during the reporting period. Estimates and assumptions are primarily made in relation to the valuation of share options, valuation allowances relating to deferred tax assets, revenue recognition, estimating clinical trial expenses and estimating reimbursements from research and development (“R&D”) tax and expenditure credits. If actual results differ from the Company’s estimates, or to the extent these estimates are adjusted in future periods, the Company’s results of operations could either benefit from, or be adversely affected by, any such change in estimate.
(c) Going concern
Management considers that there are no conditions or events, in the aggregate, that raise substantial doubt about the entity’s ability to continue as a going concern for a period of at least one year from the date the financial statements are issued. This evaluation is based on relevant conditions and events that are known and reasonably knowable at the date that the financial statements are issued, including:
a. The Company’s current financial condition, including its liquidity sources
b. The Company’s conditional and unconditional obligations due or anticipated within one year
F-9
Table of Contents
c. The funds necessary to maintain the Company’s operations considering its current financial condition, obligations, and other expected cash flows, and
d. Other conditions and events, when considered in conjunction with the above that may adversely affect the Company’s ability to meet its obligations.
(d) Reclassifications
Property and insurance costs relating to research and development facilities of $1,377,000 and $1,162,000 in the six months ended December 31, 2015 and the year ended June 30, 2015, respectively, were misclassified as general and administrative expenses in prior periods. These costs have been presented within research and development in the current period and the Company has reclassified prior period expenses to conform the presentation to the current period.
Legal expenses for patent applications of $149,000, $303,000 and $171,000 in the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively, were misclassified as research and development expenditure in prior periods. These expenses have been presented within general administrative expenses in the current period and the Company has reclassified prior period expenses to conform the presentation to the current period.
The Company has assessed the materiality of the classification errors in prior periods in accordance with the SEC’s guidance on assessing materiality, Staff Accounting Bulletin No. 99, Materiality, and determined that the errors are quantitatively and qualitatively not material.
The operating expenses for comparative periods as previously reported and as presented after the reclassifications are as follows (in thousands):
|
|
|
Six months ended
December 31, 2015 |
|
Year ended
June 30, 2015 |
|
Year ended
June 30, 2014 |
|
|
|
|
As previously
reported |
|
After
reclassification |
|
As previously
reported |
|
After
reclassification |
|
As previously
reported |
|
After
reclassification |
|
|
Research and development |
|
$ |
24,244 |
|
$ |
25,472 |
|
$ |
23,278 |
|
$ |
24,137 |
|
$ |
9,746 |
|
$ |
9,575 |
|
|
General and administrative |
|
11,145 |
|
9,917 |
|
11,234 |
|
10,375 |
|
2,600 |
|
2,771 |
|
|
Total operating expenses |
|
$ |
35,389 |
|
$ |
35,389 |
|
$ |
34,512 |
|
$ |
34,512 |
|
$ |
12,346 |
|
$ |
12,346 |
|
(e) Foreign currency
The reporting currency of the Company is the U.S. dollar. The Company has determined the functional currency of the ultimate parent company, Adaptimmune Therapeutics plc, is U.S. dollars because it predominately raises finance and expends cash in U.S. dollars. The functional currency of subsidiary operations is the applicable local currency. Transactions in foreign currencies are translated into the functional currency of the subsidiary in which they occur at the foreign exchange rate in effect on at the date of the transaction. Monetary assets and liabilities denominated in foreign currencies at the balance sheet date are translated into the functional currency of the relevant subsidiary at the foreign exchange rate in effect on the balance sheet date. Foreign exchange differences arising on translation are recognized within other income (expense) in the consolidated statement of operations.
The results of operations for subsidiaries, whose functional currency is not the U.S. dollar, are translated at an average rate for the period where this rate approximates to the foreign exchange rates ruling at the dates of the transactions and the balance sheet are translated at foreign exchange rates ruling at the balance sheet date. Exchange differences arising from this translation of foreign operations are reported as an item of other comprehensive income (loss).
The aggregate foreign currency transaction gain included in determining net income was $1,002,000, $12,596,000, $11,200,000 and $254,000 for the year ended December 31, 2016, the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively.
(f) Fair value measurements
The Company is required to disclose information on all assets and liabilities reported at fair value that enables an assessment of the inputs used in determining the reported fair values. The fair value hierarchy prioritizes valuation inputs based on the observable nature of those inputs. The hierarchy defines three levels of valuation inputs:
Level 1 — Quoted prices in active markets for identical assets or liabilities
F-10
Table of Contents
Level 2 — Inputs other than quoted prices included within Level 1 that are observable for the asset or liability, either directly or indirectly
Level 3 — Unobservable inputs that reflect the Company’s own assumptions about the assumptions market participants would use in pricing the asset or liability
The Company’s financial instruments consist primarily of cash and cash equivalents, short-term deposits, restricted cash, accounts receivable, accounts payable and accrued expenses. The carrying amounts of the Company’s financial instruments approximate fair value because of the short-term nature of these instruments.
(g) Accumulated other comprehensive income (loss)
Accumulated other comprehensive income (loss) consists of foreign currency translation adjustments. There were no reclassifications out of other comprehensive income during the periods presented.
(h) Cash, cash equivalents and restricted cash
The Company considers all highly-liquid investments with a maturity at acquisition date of three months or less to be cash equivalents. Cash and cash equivalents comprise cash balances and deposits with maturities of three months or less.
The Company’s restricted cash consists of cash providing security for letters of credit in respect of lease agreements.
The following table provides a reconciliation of cash, cash equivalents, and restricted cash reported within the balance sheet that sum to the total of the same such amounts shown in the statement of cash flows (in thousands).
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
|
|
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
158,779 |
|
$ |
194,263 |
|
$ |
229,046 |
|
|
Restricted cash |
|
4,017 |
|
4,508 |
|
— |
|
|
Total cash, cash equivalents, and restricted cash shown in the statement of cash flows |
|
$ |
162,796 |
|
$ |
198,771 |
|
$ |
229,046 |
|
(i) Short-term deposits
Short-term deposits consist of bank deposits with a maturity at acquisition date of between three and twelve months.
(j) Accounts receivable
Accounts receivable are amounts due from customers. At December 31, 2016, the Company had one customer, which was Glaxosmithkline, or GSK.
Management analyses current and past due accounts and determines if an allowance for uncollectible accounts is required based on collection experience and other relevant information. At December 31, 2016, the allowance for doubtful accounts is $nil. The process of estimating the uncollectible accounts involves assumptions and judgments and the ultimate amounts of uncollectible accounts receivable could be in excess of the amounts provided.
(k) Clinical materials
Clinical materials for use in research and development with alternative future use are capitalized as either other current assets or other non-current assets, depending on the timing of their expected consumption.
(l) Property, plant and equipment
Property, plant and equipment is stated at cost, less any impairment losses, less accumulated depreciation.
Depreciation is computed using the straight-line method over the estimated useful lives of the related assets. The following table provides the range of estimated useful lives used for each asset type:
F-11
Table of Contents
|
Computer equipment |
|
3 to 5 years |
|
|
Laboratory equipment |
|
5 years |
|
|
Office equipment |
|
5 years |
|
|
Leasehold improvements |
|
the expected duration of the lease |
|
Assets under construction are not depreciated until the asset is available and ready for its intended use.
The Company assesses property, plant and equipment for impairment whenever events or changes in circumstances indicate that an asset’s carrying amount may not be recoverable.
(m) Intangibles
Intangibles includes intellectual property (“IP”) rights for licensed technology used in research and development with an alternative future use, which are recorded at cost and amortized over the estimated useful life of the related product.
The weighted-average amortization period for IP rights for licensed technology at December 31, 2016 is seven years.
Intangibles also include acquired computer software licenses, which are recorded at cost and amortized over the estimated useful lives of approximately three years.
Intangibles are assessed for impairment whenever events or changes in circumstances indicate that an asset’s carrying amount may not be recoverable.
(n) Segmental reporting
Operating segments are identified as components of an enterprise about which separate discrete financial information is available for evaluation by the chief operating decision-maker in making decisions regarding resource allocation and assessing performance. The Company’s chief operating decision maker (the “CODM”), its chief executive officer, manages the Company’s operations on an integrated basis for the purposes of allocating resources. When evaluating the Company’s financial performance, the CODM reviews total revenues, total expenses and expenses by function and the CODM makes decisions using this information on a global basis. Accordingly, the Company has determined that it operates in one operating segment.
(o) Revenue
Revenue is recognized when earned and realized or realizable, which is generally when persuasive evidence of an arrangement exists, delivery has occurred or services have been rendered, the seller’s price to the buyer is fixed or determinable, and collectability is reasonably assured. Where applicable, all revenues are stated net of value added and similar taxes.
The Company’s revenue currently arises from a collaboration and license agreement with GSK entered into in May 2014 and amended in February 2016 (the “GSK Collaboration and License Agreement”), which requires the Company to provide multiple deliverables to GSK. The Company recognizes revenue for arrangements with multiple deliverables by identifying the separable deliverables within the arrangement, whereby a deliverable is considered separable if it has value to the customer on a standalone basis. Contingent deliverables, such as the right to nominate further development targets, which represent a substantive option (i.e. the customer is not required or compelled to purchase the optional products or services) and not priced at a significant and incremental discount are not considered to be a deliverable at inception of the arrangement.
The non-contingent arrangement consideration is allocated between the separate deliverables using the relative selling price. The relative selling price is determined using vendor-specific objective evidence (“VSOE”), if available, third party evidence if VSOE is not available, or a best estimate of the standalone selling price if neither VSOE nor third party evidence is available. The best estimate of the selling price is estimated after considering all reasonably available information, including market data and conditions, entity-specific factors such as the cost structure of the deliverable, internal profit and pricing objectives and the stage of development, if appropriate. Revenue allocated to each deliverable is recognized as it is delivered. Where delivery occurs over time, revenue is systematically recognized over the period which the Company will be providing services.
Amounts received prior to satisfying the revenue recognition criteria are recorded as deferred revenue in the Company’s consolidated balance sheet. Amounts expected to be recognized as revenue within the 12 months following the balance sheet date are classified as deferred revenue in current liabilities. Amounts not expected to be recognized as revenue within the 12 months following the balance sheet date are classified as deferred revenue, non-current.
Milestone payments which are non-refundable, non-creditable and contingent on achieving clinical milestones are recognized as revenues either on achievement of such milestones if the milestones are considered substantive or over the period the Company has
F-12
Table of Contents
continuing performance obligations, if the milestones are not considered substantive. When determining if a milestone is substantive, the Company considers the following factors:
· The degree of certainty in achieving the milestone,
· The frequency of milestone payments,
· The Company’s efforts, which result in achievement of the milestone,
· The amount of the milestone payment relative to the other deliverables and payment terms, and
· Whether the milestone payment is related to future performance or deliverables.
(p) Research and development expenditure
Research and development expenditures are expensed as incurred.
Expenses related to clinical trials are recognized as services are received. Nonrefundable advance payments for services are deferred and recognized in the consolidated statement of operations as the services are rendered. This determination is based on an estimate of the services received and there may be instances when the payments to vendors exceed the level of services provided resulting in a prepayment of the clinical expense. If the actual timing of the performance of services varies from our estimate, the accrual or prepaid expense is adjusted accordingly.
Upfront and milestone payments to third parties for in-licensed products or technology which has not yet received regulatory approval and which does not have alternative future use in R&D projects or otherwise are expensed as incurred. The Company expensed acquired in-process R&D of $3.0 million, $2.5 million, $- and $- in the year ended December 31, 2016, the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively.
Milestone payments made to third parties either on or subsequent to regulatory approval are capitalized as an intangible asset and amortized over the remaining useful life of the product.
Research and development expenditure is presented net of reimbursements from grants and R&D tax and expenditure credits from the U.K. government, which are recognized over the period necessary to match the reimbursement with the related costs when it is probable that the Company has complied with any conditions attached and will receive the reimbursement. Grant income was $414,000, $905,000, $613,000 and $241,000 in the year ended December 31, 2016, the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively. Reimbursable R&D tax and expenditure credits were $6,891,000, $1,506,000, $1,497,000 and $1,027,000 in the year ended December 31, 2016, the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively.
(q) Operating leases
Costs in respect of operating leases are charged to the consolidated statement of operations on a straight line basis over the lease term. Rent holidays are recognized on a straight-line basis over the lease term (including any rent holiday period). Lease incentives, including leasehold improvement incentives or allowances, are recorded as deferred rent and amortized as reductions to lease expense over the lease term. Leasehold improvements made by a lessee that are funded by landlord incentives or allowances are recorded as leasehold improvement assets and amortized over the shorter of the useful life of the asset and the non-cancellable lease term.
In July 2015, the Company entered into a 15 year lease agreement, with an early termination option at 123 months, for offices and research facilities in Philadelphia, U.S. The lease commenced upon completion of construction in October 2016.
In September 2015, the Company entered into an agreement for a 25-year lease, with early termination options, for a research and development facility in Oxfordshire, U.K. In October 2016, the Company entered into the lease for that facility following the completion of construction.
(r) Share-based compensation
The Company awards certain employees and nonemployees options over the ordinary shares of the parent company. The cost of share-based awards issued to employees are measured at the grant-date fair value of the award and recognized as an expense
F-13
Table of Contents
over the requisite service period. The fair value of the options is determined using the Black-Scholes option-pricing model. Share options with graded-vesting schedules are recognized on a straight-line basis over the requisite service period for each separately vesting portion of the award. The Company has elected to account for forfeitures of stock options when they occur by reversing compensation cost previously recognized, in the period the award is forfeited, for an award that is forfeited before completion of the requisite service period.
The Company has awarded share options to nonemployees for consultancy services. These share options are measured at the fair value of the goods/services received or the fair value of the equity instrument issued, whichever is more reliably measured, and then remeasured at the then-current fair values at each reporting date until the share options have vested and recognized as an expense over the requisite service period.
(s) Retirement benefits
The Company operates a defined contribution pension scheme for its directors and employees. The contributions to this scheme are expensed to the consolidated statement of operations as they fall due. The pension contributions for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014 were $976,000, $122,000, $240,000 and $139,000, respectively.
(t) Income taxes
Income taxes for the period comprise current and deferred tax. Income tax is recognized in the consolidated statement of operations except to the extent that it relates to items recognized either in other comprehensive income or directly in equity, in which case it is recognized in other comprehensive income or equity.
Current tax is the expected tax payable or receivable on the taxable income or loss for the current or prior periods using tax rates enacted at the balance sheet date.
Deferred tax is accounted for using the asset and liability method that requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of temporary differences between the financial statement carrying amount and the tax bases of assets and liabilities at the applicable tax rates. A valuation allowance is provided when it is more likely than not that some portion or all of the deferred tax assets will not be realized. The Company evaluates the realizability of its deferred tax assets by assessing its valuation allowance and by adjusting the amount of such allowance, if necessary. The factors used to assess the likelihood of realization include the Company’s forecast of future taxable income, carryback availability, reversing taxable temporary differences and available tax planning strategies that could be implemented to realize the deferred tax assets.
Income tax positions must meet a more-likely-than-not recognition threshold to be recognized. Income tax positions that previously failed to meet the more-likely-than-not threshold are recognized in the first subsequent financial reporting period in which that threshold is met. Previously recognized tax positions that no longer meet the more-likely-than-not threshold are derecognized in the first subsequent financial reporting period in which that threshold is no longer met. Recognized income tax positions are measured at the largest amount that is greater than 50 percent likely of being realized. We recognize potential accrued interest and penalties related to unrecognized tax benefits within the consolidated statement of operations as income tax expense.
In interim periods, the income tax expense (benefit) related to income (loss) from continuing operations before income tax expense (benefit) excluding significant unusual or infrequently occurring items is computed at an estimated annual effective tax rate and the tax expense (benefit) related to all other items is individually computed and recognized when the items occur.
(u) Preferred shares
In September 2014, Adaptimmune Limited issued 1,758,418 Series A Preferred Shares for net consideration of $98,872,000 after the deduction of fees of $4,949,000. On February 23, 2015, 1,758,418 Series A Preferred Shares were exchanged for newly issued Series A Preferred Shares of Adaptimmune Therapeutics Limited on a one-for-100 basis. The Series A Preferred Shares were convertible into ordinary shares at the option of the holder at an initial rate of 1:1 reducing to 2:1 on the third anniversary of the issuance, or on the occurrence of an initial public offering at a rate of 1:1 reducing from 1:1 on the first anniversary of the issuance to 2:1 on the third anniversary of the issuance.
F-14
Table of Contents
The Series A Preferred Shares contained a beneficial conversion feature, which is recognized within additional paid-in capital and accreted over the minimum period in which the investor can recognize that return. The beneficial conversion feature was accreted through a deemed dividend of $14,735,000 in the year ended June 30, 2015. The Series A Preferred Shares were converted into ordinary shares at a rate of 1:1 immediately prior to the Company’s initial public offering on NASDAQ in May 2015. Upon conversion the Company reclassified the carrying amount of the Series A Preferred Shares to common stock and additional paid-in capital.
(v) Loss per share
Basic loss per share is determined by dividing net loss attributable to ordinary shareholders by the weighted average number of ordinary shares outstanding during the period. Diluted loss per share is determined by dividing net loss attributable to ordinary shareholders by the weighted average number of ordinary shares outstanding during the period, adjusted for the dilutive effect of all potential ordinary shares that were outstanding during the period. Potentially dilutive shares are excluded when the effect would be to increase diluted earnings per share or reduce diluted loss per share.
The following table reconciles the numerator and denominator in the basic and diluted loss per share computation (in thousands):
|
|
|
Year ended
December 31,
2016 |
|
Six months
ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
Numerator for basic and diluted loss per share |
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(71,579 |
) |
$ |
(23,000 |
) |
$ |
(22,058 |
) |
$ |
(11,601 |
) |
|
Deemed dividend on convertible preferred shares |
|
— |
|
— |
|
(14,735 |
) |
— |
|
|
Net loss attributable to ordinary shareholders |
|
$ |
(71,579 |
) |
$ |
(23,000 |
) |
$ |
(36,793 |
) |
$ |
(11,601 |
) |
|
|
|
|
|
|
|
|
|
|
|
|
Denominator for basic and diluted loss per share |
|
|
|
|
|
|
|
|
|
|
Weighted average number of shares used to calculate basic and diluted loss per share |
|
424,713,997 |
|
424,711,900 |
|
214,704,593 |
|
148,335,529 |
|
The effects of the following potentially dilutive equity instruments have been excluded from the diluted loss per share calculation because they would have an antidilutive effect on the loss per share for the period:
|
|
|
Year ended
December 31,
2016 |
|
Six months
ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Weighted average number of share options(1) |
|
45,882,791 |
|
31,203,477 |
|
31,473,477 |
|
10,057,700 |
|
|
Weighted average number of Preferred Shares(2) |
|
— |
|
— |
|
122,848,381 |
|
— |
|
(1) The Company granted a total of 15,543,040 options from January 1, 2017 through to March 8, 2017.
(2) Adaptimmune Limited issued 1,758,418 Series A Preferred Shares in September 2014. In April 2015, as part of the Company reorganization, the Series A Preferred Shares of Adaptimmune Limited were exchanged for Series A Preferred Shares of Adaptimmune Therapeutics Limited on a one-for-100 basis. The Series A Preferred Shares were converted into ordinary shares at a rate of 1:1 immediately prior to the Company’s initial public offering on NASDAQ in May 2015.
(w) Related parties
Adaptimmune and Immunocore Limited (“Immunocore”) have a shared history, some overlap in board membership (which ceased on December 31, 2016) and substantial overlap in shareholder base. The Company has entered into several agreements with Immunocore regarding the shared use of certain services including licensing and research collaboration.
During the periods presented Immunocore and the Company have invoiced each other in respect of a transitional services agreement (under which certain staff resources and other administration services are supplied by each company to the other company for a transitional period). Additionally, during the periods presented Immunocore has invoiced the Company in respect of services provided under a target collaboration agreement (under which certain target identification services were provided by Immunocore), costs related to joint patents and in respect of property rent.
F-15
Table of Contents
The target collaboration agreement between Immunocore and the Company was terminated, by mutual consent, effective March 1, 2017. The companies entered into the target collaboration agreement in January 2015, to facilitate joint target identification activities and specific T-cell cloning work, and jointly create a target database of peptides. Both companies will continue to have access to the target database and associated target information after termination of the target collaboration agreement. The Company now has its own dedicated target identification capability and as a result has no requirement for ongoing target collaboration with Immunocore. The companies’ decision to end the target collaboration agreement has no impact on other agreements between them. In particular, the companies will continue to co-own the patents, patent applications and know-how relating to the underlying core TCR technology under a previously executed and irrevocable assignment and license agreement.
New accounting pronouncements
Adopted in the period
Restricted Cash
The Company has adopted Accounting Standards Update (“ASU”) 2016-18 - Statement of Cash Flows: Restricted Cash issued by the Financial Accounting Standards Board (“FASB”) in November 2016, which amends the presentation of restricted cash within the statement of cash flows. The guidance requires that the statement of cash flows explain the change during the period in the total of cash, cash equivalents, and amounts generally described as restricted cash or restricted cash equivalents rather than only cash and cash equivalents, as previously required. The guidance has been adopted retrospectively to all periods presented, which has resulted in a decrease in net cash used in investing activities of $4,666,000 in the six months ended December 31, 2015. The total of cash, cash equivalents and restricted cash is described in Note 2(h). The adoption of the guidance did not have any impact on the Company’s financial position or result of operations.
Classification of certain cash receipts and cash payments
The Company has adopted ASU 2016-15 - Statement of Cash Flows - Classification of Certain Cash Receipts and Cash Payments, issued by the FASB in August 2016, which provides clarification on the classification of certain cash receipts and cash payments where current U.S. GAAP either is unclear or does not include specific guidance. The guidance has been adopted using a retrospective transition method to all periods presented. The adoption of the guidance did not have any impact on the Company’s financial position, result of operations or cash flows.
Customer’s accounting for fees paid in a cloud computing arrangement
The Company has adopted Accounting Standards Update 2015-05 - Internal-Use Software: Customer’s Accounting for Fees Paid in a Cloud Computing Arrangement issued by the FASB in April 2015, which clarifies a customer’s accounting for fees paid in a cloud computing arrangement. The guidance considers whether a cloud computing arrangement includes a software license and clarifies that the customer should account for the software license element of the arrangement consistent with the acquisition of other software licenses. If a cloud computing arrangement does not include a software license, the customer should account for the arrangement as a service contract. The guidance has been adopted prospectively to all arrangements entered into or materially modified after January 1, 2016. The adoption of this guidance did not have any impact on the Company’s financial position, results of operations or cash flows.
To be adopted in future periods
Intra-Entity Transfers of Assets Other Than Inventory
In October 2016, the FASB issued ASU 2016-16 - Income Taxes: Intra-Entity Transfers of Assets Other Than Inventory, which requires that entities recognize the income tax consequences of an intra-entity transfer of an asset other than inventory when the transfer occurs. The guidance is effective for annual reporting periods beginning after December 15, 2017, including interim reporting periods within those annual reporting periods. Early adoption is permitted for all entities as of the beginning of an annual reporting period for which financial statements (interim or annual) have not been issued or made available for issuance. The guidance should be applied on a modified retrospective basis through a cumulative-effect adjustment directly to retained earnings as of the beginning of the period of adoption. The Company does not believe the adoption of the guidance will have a material impact on the consolidated financial statements.
F-16
Table of Contents
Accounting for leases
In February 2016, the FASB issued ASU 2016-02 - Leases. The guidance requires that lessees recognize a lease liability, which is a lessee’s obligation to make lease payments arising from a lease, measured on a discounted basis; and a right-of-use asset, which is an asset that represents the lessee’s right to use, or control the use of, a specified asset for the lease term at the commencement date. The guidance also makes targeted improvements to align lessor accounting with the lessee accounting model and guidance on revenue from contracts with customers. The guidance is effective for the fiscal year beginning January 1, 2019, including interim periods within that fiscal year. Early application is permitted. The guidance must be adopted on a modified retrospective transition approach for leases existing, or entered into after, the beginning of the earliest comparative period presented in the financial statements. The Company is currently evaluating the impact of the guidance on the consolidated financial statements.
Recognition and measurement of financial assets and financial liabilities
In January 2016, the FASB issued ASU 2016-01 - Financial Instruments - Overall: Recognition and Measurement of Financial Assets and Financial Liabilities, which amended the guidance on the recognition and measurement of financial assets and financial liabilities. The new guidance requires that equity investments (except those accounted for under the equity method of accounting, or those that result in consolidation of the investee) are measured at fair value with changes in fair value recognized in net income. The guidance also requires the use of an exit price when measuring the fair value of financial instruments for disclosure purposes, eliminates the requirement to disclose the methods and significant assumptions used to estimate the fair value that is required to be disclosed for financial instruments measured at amortized cost and requires separate presentation of financial assets and financial liabilities by measurement category and form of financial asset. The guidance is effective for the fiscal year beginning January 1, 2018, including interim periods within that fiscal year. The Company does not believe the adoption of the guidance will have a material impact on the consolidated financial statements.
Revenue from contracts with customers
In May 2014, the FASB issued ASU 2014-09 - Revenue from Contracts with Customers which requires a new approach to revenue recognition and in March, April, May and December 2016, the FASB issued additional clarification related to this guidance. The core principle of the guidance is that an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. To achieve that core principle, an entity should apply the following steps:
Step 1: Identify the contract(s) with a customer.
Step 2: Identify the performance obligations in the contract.
Step 3: Determine the transaction price.
Step 4: Allocate the transaction price to the performance obligations in the contract.
Step 5: Recognize revenue when (or as) the entity satisfies a performance obligation.
The guidance is effective for the fiscal year beginning January 1, 2018, including interim reporting periods within that reporting period. Earlier application is permitted. The Company intends to adopt the guidance with effect from January 1, 2018. The guidance can be adopted retrospectively to each prior reporting period presented, subject to certain practical expedients, or retrospectively with the cumulative effect of initially applying the guidance recognized at the date of initial application.
The Company is in the process of assessing the impact of the guidance as it relates to the GSK Collaboration and License Arrangement. The Company’s preliminary assessment is substantially complete but there are several complex issues that are being considered. Once these issues are resolved, the Company will determine the transition method which will be applied and evaluate the disclosure requirements. The adoption of ASU 2014-09 may have a material effect on the Company’s financial statements but the quantitative effect cannot be reasonably estimated at this time. The Company continues to monitor additional changes, modifications, clarifications or interpretations undertaken by the FASB, which may impact its assessment.
Note 3 — Revenue
GSK Collaboration and License Agreement
Revenue represents recognized income from the GSK Collaboration and License Agreement. The GSK Collaboration and License Agreement contains the following significant deliverables, which are separate accounting units: (i) the development of, and option to obtain an exclusive license to, the Company’s NY-ESO SPEAR T-cells, and (ii) the development of, and option to obtain an exclusive license to a second target, PRAME. In addition, GSK also has the right to nominate three additional target peptides, excluding those where the Company has already initiated development of a SPEAR T-cell candidate, which is not considered to be a deliverable at the inception of the arrangement because it represents a substantive option not
F-17
Table of Contents
priced at a significant and incremental discount. The Company received an upfront payment of $42.1 million (£25 million) in June 2014 and has achieved non-substantive development milestones of $17.4 million in the year ended December 31, 2016, $14.4 million in the six months ended December 31, 2015 and $7.2 million in the year ended June 30, 2015. The Company is entitled to further non-substantive milestone payments based on the achievement of specified development milestones by the Company. When, and if, GSK exercises its option to obtain an exclusive license to a target, an option exercise fee will be payable and the Company will be entitled to further development and commercialization milestone payments based on achievement of specified milestones by GSK. The non-contingent arrangement consideration was allocated between the separate deliverables using the Company’s best estimate of the relative selling price. In determining the best estimate, the Company considered internal pricing objectives it used in negotiating the GSK Collaboration and License Agreement together with internal data regarding the cost of providing services for each deliverable.
In addition to the development milestones, the Company is entitled to royalties from GSK on all GSK sales of TCR therapeutic products licensed under the agreement, varying between a mid-single-digit percentage and a low-double-digit percentage of net sales. No royalties have been received as of December 31, 2016. Sales milestones also apply once any TCR therapeutic covered by the GSK Collaboration and License Agreement is on the market.
The GSK Collaboration and License Agreement is effective until all payment obligations expire. The agreement can also be terminated on a collaboration program-by-collaboration program basis by GSK for lack of feasibility or inability to meet certain agreed requirements. Both parties have rights to terminate the agreement for material breach upon 60 days’ written notice or immediately upon insolvency of the other party. GSK has additional rights to terminate either the agreement or any specific license or collaboration program on provision of 60 days’ notice to us. The Company also has rights to terminate any license where GSK ceases development or withdraws any licensed TCR therapeutic in specified circumstances.
In February 2016, the terms of the GSK Collaboration and License Agreement were expanded to accelerate the development of the Company’s NY-ESO SPEAR T-cells towards pivotal trials in synovial sarcoma, as well as the exploration of development of NY-ESO SPEAR T-cells in myxoid round-cell liposarcoma. The amendment also provides the opportunity for up to eight combination studies using NY-ESO SPEAR T-cells and increases the potential development milestones that the Company is eligible to receive. These development milestones will be allocated to the separate standalone deliverables within the arrangement once the milestone is achieved.
The revenue recognized to date relates to the upfront fee and non-substantive development milestones payments received, which are being recognized using the proportional performance model in revenue systematically over the period in which the Company is delivering services under the GSK Collaboration and License Agreement, which is determined to be the period until GSK’s option to obtain licenses expires. We regularly review and monitor the performance of the GSK Collaboration and License Agreement to determine the period over which we will be delivering services to GSK. The Company recognized revenue of $14,198,000, $8,979,000, $9,871,000 and $825,000 in the year ended December 31, 2016, the six months ended December 31, 2015 and years ended June 30, 2015 and 2014, respectively.
The Company regularly reviews, and when a change in facts or circumstances occurs, adjusts the estimate of the period over which the Company will deliver services under the GSK Collaboration and License Agreement. In prior periods this has not resulted in a significant impact on revenue recognized. However, in June and December 2016, the estimate of the period over which the Company will deliver services under the GSK Collaboration and License Agreement was increased due to a change in facts and circumstances. These changes in estimate resulted in a decrease in revenue of $5,615,000 in the year ended December 31, 2016 compared to the revenue that would have been recognized based on previous estimates. The changes in estimate will also result in a decrease in revenue amortization of $2,237,000 in the year ended December 31, 2017 and an increase in revenue amortization of $939,000, $900,000 and $6,053,000 in the years ended December 31, 2018, 2019 and 2020, respectively, compared to the revenue that would have been recognized based on previous estimates.
Note 4 — Financial instruments
The Company’s financial instruments consist primarily of cash and cash equivalents, short-term deposits, restricted cash, accounts receivable, accounts payable and accrued expenses. The carrying amounts of the Company’s financial instruments approximate to the fair value because of the short-term nature of these instruments.
Significant concentration of credit risk
The Company held cash and cash equivalents of $158,779,000, short-term deposits of $22,694,000 and restricted cash of $4,017,000 at December 31, 2016. The cash and cash equivalents, short-term deposits and restricted cash are held with multiple banks and the Company monitors the credit rating of those banks.
F-18
Table of Contents
The Company has one customer as a result of the Collaboration and License Agreement with GSK. The Company has been transacting with GSK since June 2014, during which time no impairment losses have been recognized. There are no amounts which are past due at December 31, 2016.
Foreign exchange risk
We are exposed to foreign exchange rate risk because we currently operate in the U.K. and the U.S. Our revenue from the GSK Collaboration and License Agreement is denominated in pounds sterling and is generated by our U.K-based subsidiary, which has a pounds sterling functional currency. As a result, these sales are subject to translation into U.S. Dollars when we consolidate our financial statements. Our expenses are generally denominated in the currency in which our operations are located, which are the U.K. and the U.S. However our U.K.-based subsidiary incurs significant research and development costs in U.S. dollars and, to a lesser extent, Euros.
The results of operations and cash flows will be subject to fluctuations due to changes in foreign currency exchange rates, which could harm our business in the future. The exchange rate as at December 31, 2016, the last business day of the reporting period, was £1.00 to $1.233. The exchange rate as at February 28, 2017 was £1.00 to $1.243. We seek to minimize this exposure by maintaining currency cash balances at levels appropriate to meet foreseeable expenses in U.S. dollars and pounds sterling. To date, we have not used forward exchange contracts or other currency hedging products to manage our exchange rate exposure, although we may do so in the future.
Note 5 - Property, plant and equipment, net
Property and equipment, net consisted of the following (in thousands):
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
|
|
|
|
|
|
|
|
|
|
Computer equipment |
|
$ |
1,904 |
|
$ |
1,182 |
|
$ |
649 |
|
|
Laboratory equipment |
|
11,423 |
|
11,016 |
|
3,547 |
|
|
Office equipment |
|
265 |
|
258 |
|
192 |
|
|
Leasehold improvements |
|
4,498 |
|
1,631 |
|
1,926 |
|
|
Assets under construction |
|
14,332 |
|
1,147 |
|
— |
|
|
|
|
32,422 |
|
15,234 |
|
6,314 |
|
|
Less accumulated depreciation |
|
(4,523 |
) |
(2,009 |
) |
(921 |
) |
|
|
|
$ |
27,899 |
|
$ |
13,225 |
|
$ |
5,393 |
|
Depreciation expense was $3,126,000, $1,176,000, $705,000 and $240,000 for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively.
The Company has disposed of leasehold improvements resulting in a loss on disposal of $122,000, which is included within general and administrative expenses in the statement of operations.
Note 6 — Intangible assets, net
Intangible assets, net consisted of the following (in thousands):
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
|
|
|
|
|
|
|
|
|
|
Acquired software licenses |
|
$ |
1,310 |
|
$ |
399 |
|
$ |
208 |
|
|
Licensed IP rights — completed technology |
|
183 |
|
— |
|
— |
|
|
|
|
1,493 |
|
399 |
|
208 |
|
|
Less accumulated amortization |
|
(225 |
) |
(94 |
) |
(30 |
) |
|
|
|
$ |
1,268 |
|
$ |
305 |
|
$ |
178 |
|
F-19
Table of Contents
Amortization expense was $160,000, $69,000, $30,000 and $nil for the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014, respectively. The estimated aggregate amortization expense in respect of these assets for each of the five years ended 2021 is $331,000, $387,000,$349,000, $116,000 and $22,000, respectively.
Note 7 — Accrued expenses and other current liabilities
Accrued expenses and other current liabilities consisted of the following (in thousands):
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
|
|
|
|
|
|
|
|
|
|
Accrued clinical and development expenses |
|
$ |
4,938 |
|
$ |
3,143 |
|
$ |
1,790 |
|
|
Accrued employee compensation and benefits payable |
|
4,539 |
|
2,748 |
|
248 |
|
|
Accrued capital expenditure |
|
3,954 |
|
42 |
|
973 |
|
|
Value added tax |
|
2,014 |
|
744 |
|
— |
|
|
Other accrued purchases |
|
1,003 |
|
841 |
|
826 |
|
|
Other current liabilities |
|
1,080 |
|
— |
|
40 |
|
|
|
|
$ |
17,528 |
|
$ |
7,518 |
|
$ |
3,877 |
|
Note 8 — Contingencies and commitments
Leases
Future minimum lease payments under operating leases at December 31, 2016 are presented below (in thousands):
|
|
|
December 31,
2016 |
|
|
2017 |
|
2,112 |
|
|
2018 |
|
2,755 |
|
|
2019 |
|
3,361 |
|
|
2020 |
|
3,245 |
|
|
2021 |
|
3,130 |
|
|
Thereafter |
|
17,983 |
|
|
|
|
$ |
32,586 |
|
|
|
|
|
|
The Company leases property under operating leases expiring through 2027. Lease expenses amounted to $2,255,000, $841,000, $610,000 and $287,000 for the year ended December 31, 2016, six months ended December 31, 2015 and years ended June 30, 2015, and 2014, respectively, which is included within research and development and general and administrative expenses in the Company’s consolidated statement of operations.
In July 2015, the Company entered into a long-term lease agreement, with an early termination option at 123 months, for offices and research facilities in Philadelphia, U.S. In October 2016, the lease commenced upon completion of construction. The related lease commitments are included in the table above.
In September 2015, the Company entered into an agreement for a 25-year lease, with early termination options, for a research and development facility in Oxfordshire, U.K. In October 2016, the Company entered into the lease for that facility following the completion of construction. The related lease commitments are included in the table above.
Capital commitments
At December 31, 2016, the Company had commitments for capital expenditure totaling $8,093,000, which the Company expects to incur within one year.
Purchase commitments for clinical materials, clinical trials and contract manufacturing
At December 31, 2016, the Company had non-cancellable commitments for purchase of clinical materials, executing and administering clinical trials, and for contract manufacturing of $50,972,000, of which the Company expects to pay $34,164,000 within
F-20
Table of Contents
one year, $8,443,000 in one to three years, $6,796,000 in three to five years, and $1,569,000 after five years. The timing of these payments varies depending on the rate of progress of development and clinical trial enrollment rates. Our subcontracted costs for clinical trials and contract manufacturing were $23,565,000, $8,585,000, $8,818,000 and $5,886,000 for the year ended December 31, 2016, six months ended December 31, 2015 and years ending June 30, 2015 and 2014, respectively.
Bellicum Pharmaceuticals Inc, Co-Development and Co-Commercialization Agreement
On December 16, 2016, the Company entered into a Co-Development and Co-Commercialization Agreement with Bellicum Pharmaceuticals, Inc. (“Bellicum”) in order to facilitate a staged collaboration to evaluate, develop and commercialize next generation T-cell therapies.
Under the agreement, the Company will evaluate Bellicum’s GoTCR technology (inducible MyD88/CD40 co-stimulation, or iMC) with our SPEAR T-cells for the potential to create enhanced T-cell therapeutics. Depending on results of the initial preclinical proof-of-concept phase, the agreement may progress to a two-target co-development and co-commercialization phase. To the extent necessary, and in furtherance of the parties’ proof-of-concept and co-development efforts, the parties granted each other a royalty-free, non-transferable, non-exclusive license covering their respective technologies for purposes of facilitating such proof—of-concept and co-development efforts. In addition, as to covered therapies developed under the agreement, the parties granted each other a reciprocal exclusive license for the commercialization of such therapies.
With respect to any joint commercialization of a covered therapy, the parties agreed to negotiate in good faith the commercially reasonable terms of a co-commercialization agreement. The parties also agreed that any such agreement shall provide for, among other things, equal sharing of the costs of any such joint commercialization and the calculation of profit shares as set forth in the agreement.
The agreement will expire on a country-by-country basis once the parties cease commercialization of the T-cell therapies covered by the agreement, unless earlier terminated by either party for material breach, non-performance or cessation of development, bankruptcy/insolvency, or failure to progress to co-development phase.
Merck Combination Agreement
On October 27, 2016, the Company entered into a clinical trial collaboration agreement with Merck (known as MSD outside the United States and Canada), for the assessment of our NY-ESO SPEAR T-cell therapy in combination with Merck’s PD-1 inhibitor, KEYTRUDA® (pembrolizumab), in patients with multiple myeloma. Under the terms of the agreement, each of Merck and the Company will manufacture and supply its relevant compound for use in the combination study. The agreement will last until the earlier of delivery of the final study report or study completion. Either party may terminate the agreement for material breach, patient safety, regulatory action preventing supply of compound or withdrawal of regulatory approval for one of the combination study compounds. Merck may also terminate the agreement where it believes its compound is being used in an unsafe manner.
MD Anderson Strategic Alliance
On September 26, 2016, the Company announced that it had entered into a multi-year strategic alliance with The University of Texas MD Anderson Cancer Center (“MD Anderson”) designed to expedite the development of T-cell therapies for multiple types of cancer. The Company and MD Anderson will collaborate in a number of studies including clinical and preclinical development of the Company’s SPEAR T-cell therapies targeting NY-ESO, MAGE-A10 and future clinical stage first and second generation SPEAR T-cell therapies such as MAGE-A4 across a number of cancers, including bladder, lung, ovarian, head and neck, melanoma, sarcoma, esophageal and gastric cancers.
Under the terms of the alliance agreement, the Company has committed funding of at least $19,644,000 to fund studies under the alliance agreement. Payment of this funding is contingent on mutual agreement to study orders, in order for any study to be included under the alliance, and the performance of set milestones by MD Anderson.
The Company will make payments to MD Anderson as certain milestones are achieved and these costs will be expensed to research and development as MD Anderson renders the services under the strategic alliance. The timing and amount of future payments is uncertain.
The alliance agreement may be terminated by either party for material breach by the other party. Individual studies may be terminated inter alia for material breach, health and safety concerns or where the institutional review board, the review board at the clinical site with oversight of the clinical study, requests termination of any study. Where any legal or regulatory authorization is finally withdrawn or terminated, the relevant study will also terminate automatically.
Universal Cells Research, Collaboration and License Agreement
On November 25, 2015, the Company entered into a Research, Collaboration and License Agreement relating to gene editing and HLA-engineering technology with Universal Cells, Inc. (“Universal Cells”). The Company paid an upfront license and start-up fee of $2.5 million to Universal Cells in November 2015 and a milestone payment of $3.0 million in February 2016. Further milestone payments of up to $44 million are payable if certain development and product milestones are achieved. Universal Cells
F-21
Table of Contents
would also receive a profit-share payment for the first product, and royalties on sales of other products utilizing its technology. The upfront and start-up fee was expensed to research and development when incurred.
ThermoFisher License Agreement
In 2012, the Company entered into a series of license and sub-license agreements with Life Technologies Corporation, part of ThermoFisher Scientific, Inc. (“ThermoFisher”) that provide the Company with a field-based exclusive license under certain intellectual property rights owned or controlled by ThermoFisher. The Company paid upfront license fees of $1.0 million relating to the license and sublicense agreements and has an obligation to pay minimum annual royalties (in the tens of thousands of U.S. dollars prior to licensed product approval and thereafter at a level of 50% of running royalties in the previous year), milestone payments and a low single-digit running royalty payable on the net selling price of each licensed product. The upfront payment made in 2012 was expensed to research and development when incurred. Subsequent milestone payments have been recognized as an intangible asset due to the technology having alternative future use in research and development projects at the time of the payment. The minimum annual royalties have been expensed as incurred.
On June 16, 2016, the Company entered into a supply agreement with ThermoFisher for the supply of the Dynabeads® CD3/CD28 technology. The Dynabeads® CD3/CD28 technology is designed to isolate, activate and expand human T-cells, and is being used in the manufacturing of the Company’s affinity enhanced T-cell therapies. The supply agreement runs until December 31, 2025. Under the supply agreement the Company is required to purchase its requirements for CD3/CD28 magnetic bead product exclusively from ThermoFisher for a period of 5 years and there are also minimum purchasing obligations, which are included within ‘Purchase commitments for clinical materials, clinical trials and contract manufacturing’ set forth above. ThermoFisher has the right to terminate the supply agreement for material breach or insolvency.
Note 9 — Stockholders’ equity
Ordinary shares
Each holder of ordinary shares is entitled to one vote, on a show of hands and one vote per share on a poll, at general meetings of the Company. On the winding up of the Company, the assets of the Company available for distribution to holders remaining after payment of all other debts and liabilities of the Company shall be paid to the shareholders in proportion to the number of shares held by each of them.
The Directors have the authority to allot new shares or to grant rights to subscribe for or to convert any security into shares in the Company up to a maximum aggregate nominal amount of £149,937 at December 31, 2016. This authority will expire on December 17, 2020.
Initial public offering
On May 11, 2015, the Company closed its IPO on NASDAQ, issuing 11,250,000 American Depositary Shares representing 67,500,000 ordinary shares with nominal value of $104,000 (£67,500) for proceeds of $175,989,000, net of issuance costs of $13,387,000.
Corporate reorganization
On April 1, 2015, the Company completed a corporate reorganization. Pursuant to the first stage of this reorganization, on February 23, 2015, all shareholders of Adaptimmune Limited exchanged each of the Series A Preferred Shares and ordinary shares held by them for newly issued Series A Preferred Shares and ordinary shares of Adaptimmune Therapeutics Limited on a one-for-100 basis, resulting in Adaptimmune Limited becoming a wholly-owned subsidiary of Adaptimmune Therapeutics Limited. On April 1, 2015, pursuant to the final step in the corporate reorganization, Adaptimmune Therapeutics Limited re-registered as a public limited company with the name Adaptimmune Therapeutics plc.
On March 20, 2015, Adaptimmune Limited share options over ordinary shares granted to directors and employees under share option plans that were in existence immediately prior to the reorganization were exchanged for share options over ordinary shares of Adaptimmune Therapeutics plc on a one-for-100 basis with no change in any of the terms or conditions.
Adaptimmune Therapeutics plc’s Board, management and corporate governance arrangements, and consolidated assets and liabilities immediately following the reorganization were the same as Adaptimmune Limited immediately before the reorganization.
F-22
Table of Contents
Convertible preferred shares
In September 2014, Adaptimmune Limited issued 1,758,418 Series A Preferred Shares for net consideration of $98,872,000 after the deduction of fees of $4,949,000. In February 2015, the Series A Preferred Shares were exchanged for Series A Preferred Shares of Adaptimmune Therapeutics Limited on a one-for-100 basis. The Series A Preferred Shares were convertible into ordinary shares at the option of the holder at an initial rate of 1:1 reducing to 2:1 on the third anniversary of the issuance, or on the occurrence of an initial public offering at a rate of 1:1 reducing from 1:1 on the first anniversary of the issuance to 2:1 on the third anniversary of the issuance.
The Series A Preferred Shares were converted into ordinary shares at a rate of 1:1 immediately prior to the Company’s initial public offering on NASDAQ in May 2015.
Note 10 — Share-based compensation
The Company grants options over ordinary shares in Adaptimmune Therapeutics plc under the following option plans: (i) the Adaptimmune Therapeutics plc Employee Share Option Scheme (adopted on 14 January 2016), (ii) the Adaptimmune Therapeutics plc 2015 Share Option Scheme and (adopted March 16, 2015) (ii) the Adaptimmune Therapeutics plc Company Share Option Plan (adopted March 16, 2015).
The Adaptimmune Therapeutics plc Company Share Option Plan is a tax efficient option scheme intended to comply with the requirements of Schedule 4 to the Income Tax (Earnings and Pensions) Act 2003 of the United Kingdom, which provides for the grant of company share option plan (“CSOP”) options. Grants may not exceed the maximum value of £30,000 per participant for the shares under the option, which is a CSOP compliance requirement.
Generally, the vesting dates for the options granted under these plans are 25% on the first anniversary of the grant date and 75% in monthly installments over the following three years. However, the options granted to non-executive directors under the Adaptimmune Therapeutics plc 2015 Share Option Scheme vest and become exercisable as follows:
|
Options granted to non-executive directors on May 11, 2015: |
|
Immediately on grant date |
|
|
|
|
|
Options granted to a non-executive director on June 23, 2016: |
|
25% on the first anniversary of the grant date and 75% in monthly installments over the following two years |
|
|
|
|
|
Options granted to non-executive directors on August 11, 2016: |
|
100% on the first anniversary of the grant date |
|
|
|
|
|
Options granted to non-executive directors on November 28, 2016: |
|
25% on the first anniversary of the grant date and 75% in monthly installments over the following two years |
Options granted under these plans are not subject to performance conditions. The contractual term of options granted under these plans is ten years.
The maximum aggregate number of options which may be granted under these plans and any incentive plans adopted by the Company cannot exceed a scheme limit that equates to 8% of the initial fully diluted share capital of the Company immediately following our IPO plus an automatic annual increase of an amount equivalent to 4% of the issued share capital on each 30 June (or such lower number as the Board, or an appropriate committee of the Board, may determine). The automatic increase is effective from July 1, 2016.
Prior to December 31, 2014, the Company granted options to purchase ordinary shares in Adaptimmune Limited under three option schemes:
(i) The Adaptimmune Limited Share Option Scheme was adopted on May 30, 2008. Under this scheme Enterprise Management Incentive (“EMI”) options (which are potentially tax-advantaged in the United Kingdom) have been granted (subject to the relevant conditions being met) to our employees who are eligible to receive EMI options under applicable U.K. tax law and unapproved options (which do not attract tax advantages) have been granted to our employees who are not eligible to receive EMI options, and to our directors and consultants. In May 2014, the Company no longer qualified for EMI status and since that date, no further EMI options were granted under this scheme; however, unapproved options have been under granted under this scheme since that date.
F-23
Table of Contents
(ii) The Adaptimmune Limited 2014 Share Option Scheme was adopted on April 11, 2014. EMI options were granted (subject to the relevant conditions being met) under this scheme to our employees who are eligible to receive EMI options under applicable U.K. tax law. Unapproved options were granted to our employees who are not eligible to receive EMI options and to directors. In May 2014, the Company no longer qualified for EMI status and since that date, no further EMI options were granted under this scheme; however, unapproved options have been under granted under this scheme since that date.
(iii) The Adaptimmune Limited Company Share Option Plan was adopted on December 16, 2014. This scheme allowed the grant of options to our eligible employees prior to the Company’s corporate reorganization. This scheme is a tax efficient option scheme and options were granted on December 19, 2014 and on December 31, 2014 to our part-time and full-time employees.
As part of the corporate reorganization in connection with our IPO, the holders of options granted under these schemes over ordinary shares of Adaptimmune Limited were granted equivalent options on substantially the same terms over ordinary shares of Adaptimmune Therapeutics plc (“Replacement Options”) in exchange for the release of these options. The Company does not intend to grant any further options under these schemes.
Generally, the vesting dates for the Replacement Options under the Adaptimmune Limited schemes are:
|
Options granted in 2009: |
|
100% on the third anniversary of the grant date |
|
|
|
|
|
Options granted in 2011, 2012, 2013 and April 2014: |
|
25% on the first anniversary of the grant date and 75% in annual installments over the following three years |
|
|
|
|
|
Options granted in December 2014: |
|
25% on the first anniversary of the grant date and 75% in monthly installments over the following three years |
The contractual life of options granted under these schemes is ten years.
In August 2016, the Company accelerated the vesting of 361,222 share options held by two non-executive directors, such that those options became vested and exercisable on December 30, 2016 when the non-executive directors stepped down from the board of directors, and the options expire on December 31, 2018.
The following table shows the total share-based compensation expense included in the consolidated statement of operations (thousands):
|
|
|
Year ended
December 31,
2016 |
|
Six months ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
4,185 |
|
$ |
1,587 |
|
$ |
5,426 |
|
$ |
121 |
|
|
General and administrative |
|
4,636 |
|
1,981 |
|
1,652 |
|
211 |
|
|
|
|
$ |
8,821 |
|
$ |
3,568 |
|
$ |
7,078 |
|
$ |
332 |
|
At December 31, 2016, December 31, 2015 and June 30, 2015, there were 3,074,600, 2,774,600 and 2,774,600 share options granted to nonemployees outstanding, respectively. These share options are measured at the current fair values at each reporting date until the share options have vested and recognized in the consolidated statement of operations over the requisite service period. The total share-based payment expense included in the consolidated statement of operations includes a benefit of $488,000 and $33,000 in the year ended December 31, 2016 and six months ended December 31, 2015, respectively, and a charge of $2,001,000 and $44,000 in the years ended 2015 and 2014, respectively relating to share options granted to nonemployees.
At December 31, 2016, there was $7,918,000 of total unrecognized compensation cost related to stock options granted but not vested under the plans. That cost will be recognized over an expected remaining weighted-average period of 0.8 years.
There were 19,404,373, 21,779,577 and 5,627,700 options granted in the years ended December 31, 2016, June 30, 2015 and 2014, respectively. No share options were granted in the six months ended December 31, 2015. The weighted average fair value of stock options granted in the years ended December 31, 2016, June 30, 2015 and 2014 were $0.74, $0.64 and $0.13, respectively.
F-24
Table of Contents
The following table summarizes all stock option activity for the year ended December 31, 2016:
|
|
|
Options |
|
Weighted
average
exercise price
per option |
|
Average
remaining
contractual
term (years) |
|
Aggregate
intrinsic value
(thousands) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Outstanding at January 1, 2016 |
|
31,203,477 |
|
£ |
0.41 |
|
|
|
|
|
|
Changes during the period: |
|
|
|
|
|
|
|
|
|
|
Granted |
|
19,404,373 |
|
£ |
0.89 |
|
|
|
|
|
|
Exercised |
|
(63,192 |
) |
£ |
0.22 |
|
|
|
|
|
|
Forfeited |
|
(1,307,368 |
) |
£ |
1.04 |
|
|
|
|
|
|
Outstanding at December 31, 2016 |
|
49,237,290 |
|
£ |
0.58 |
|
8.2 |
|
$ |
8,205 |
|
|
Exercisable at December 31, 2016 |
|
17,167,747 |
|
£ |
0.41 |
|
7.5 |
|
$ |
4,906 |
|
The following table summarizes information about stock options outstanding as of December 31, 2016:
|
Outstanding |
|
Exercisable |
|
|
Exercise price |
|
Total share options |
|
Weighted-average
remaining
contractual life |
|
Weighted-average
exercise price |
|
Total share options |
|
Weighted-average
exercise price |
|
|
£ |
0 – 0.25 |
|
9,858,104 |
|
6.6 |
|
£ |
0.11 |
|
6,482,204 |
|
£ |
0.11 |
|
|
0.26 – 0.50 |
|
19,156,064 |
|
8.1 |
|
0.42 |
|
8,975,893 |
|
0.42 |
|
|
0.51 – 0.75 |
|
1,646,000 |
|
9.9 |
|
0.58 |
|
— |
|
— |
|
|
0.76 – 1.00 |
|
15,493,264 |
|
9.5 |
|
0.93 |
|
559,049 |
|
0.89 |
|
|
1.01 – 1.50 |
|
1,498,243 |
|
9.4 |
|
1.06 |
|
— |
|
— |
|
|
1.51 – 2.00 |
|
1,585,615 |
|
8.4 |
|
1.82 |
|
1,150,601 |
|
1.82 |
|
|
Total |
|
49,237,290 |
|
8.2 |
|
£ |
0.58 |
|
17,167,747 |
|
£ |
0.41 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
There were 63,192 and 2,265,000 share options exercised in the years ended December 31, 2016 and June 30, 2014, respectively. No share options were exercised in the six months ended December 31, 2015 and year ended June 30, 2015. In the year ended December 31, 2016 the total intrinsic value of stock options exercised was $40,000 and the cash received from exercise of stock options was $17,000. In the year ended June 30, 2014 the total intrinsic value of stock options exercised was $130,000 and the cash received from exercise of stock options was $192,000. The Company recognizes tax benefits arising on the exercise of stock options regardless of whether the benefit reduces current taxes. The tax benefit arising on the exercise of stock options was $8,000 for the year ended December 31, 2016 and nil for the six months ended December 31, 2015 and the years ended June 30, 2015 and 2014. The Company satisfies the exercise of stock options through newly issued shares.
The fair value of the stock options granted during the period was calculated using the Black-Scholes option-pricing model using the following assumptions:
|
|
|
Year ended
December 31,
2016 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
Expected term (years) |
|
5 years |
|
5 years |
|
5 years |
|
|
Expected volatility |
|
68-73% |
|
60% |
|
60% |
|
|
Risk free rate |
|
0.17-1.07% |
|
1.04-1.54% |
|
1.73% |
|
|
Expected dividend yield |
|
0% |
|
0% |
|
0% |
|
The expected term of the option is based on management judgment. Due to the Company’s lack of sufficient history as a publicly traded company, management’s estimate of expected volatility is based on the average volatilities of seven public companies with similar attributes to the Company. The risk free rate is based on the Bank of England’s estimates of gilt yield curve as of the respective grant dates.
F-25
Table of Contents
Note 11 — Income taxes
Loss before income taxes is as follows (in thousands):
|
|
|
Year ended
December 31,
2016 |
|
Six months ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
U.S. |
|
$ |
(3,373 |
) |
$ |
(1,771 |
) |
$ |
(1,108 |
) |
$ |
1,941 |
|
|
U.K. |
|
(67,314 |
) |
(21,284 |
) |
(20,706 |
) |
(13,467 |
) |
|
Loss before income taxes |
|
(70,687 |
) |
$ |
(23,055 |
) |
$ |
(21,814 |
) |
$ |
(11,526 |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The components of income tax expense (benefit) are as follows (in thousands):
|
|
|
Year ended
December 31,
2016 |
|
Six months ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
United States: |
|
|
|
|
|
|
|
|
|
|
Federal |
|
$ |
752 |
|
$ |
33 |
|
$ |
121 |
|
$ |
75 |
|
|
State and local |
|
140 |
|
(88 |
) |
123 |
|
— |
|
|
U.K. |
|
— |
|
— |
|
— |
|
— |
|
|
Total current tax expense (benefit) |
|
$ |
892 |
|
$ |
(55 |
) |
$ |
244 |
|
$ |
75 |
|
|
|
|
|
|
|
|
|
|
|
|
|
United States: |
|
|
|
|
|
|
|
|
|
|
Federal |
|
— |
|
— |
|
— |
|
— |
|
|
State and local |
|
— |
|
— |
|
— |
|
— |
|
|
U.K. |
|
— |
|
— |
|
— |
|
— |
|
|
Total deferred tax expense (benefit) |
|
— |
|
— |
|
— |
|
— |
|
|
Total income tax expense (benefit) |
|
$ |
892 |
|
$ |
(55 |
) |
$ |
244 |
|
$ |
75 |
|
At December 31, 2016, December 31, 2015 and June 30, 2015 the tax effects of temporary differences that give rise to deferred tax assets and liabilities were as follows (in thousands):
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
|
|
|
|
|
|
|
|
|
|
Property, plant and equipment: |
|
$ |
(1,880 |
) |
$ |
(2,080 |
) |
$ |
(888 |
) |
|
Accruals |
|
(326 |
) |
(8 |
) |
— |
|
|
Deferred tax liabilities |
|
(2,206 |
) |
(2,088 |
) |
(888 |
) |
|
|
|
|
|
|
|
|
|
|
Share-based compensation expense |
|
4,632 |
|
2,721 |
|
1,557 |
|
|
Intangible assets |
|
348 |
|
443 |
|
— |
|
|
Deferred rent |
|
144 |
|
— |
|
— |
|
|
Deferred revenue |
|
— |
|
— |
|
115 |
|
|
Other accruals |
|
82 |
|
37 |
|
30 |
|
|
Net operating loss and expenditure credit carryforwards |
|
14,613 |
|
8,318 |
|
7,508 |
|
|
Deferred tax assets |
|
19,819 |
|
11,519 |
|
9,210 |
|
|
Valuation allowance |
|
(17,613 |
) |
(9,431 |
) |
(8,322 |
) |
|
|
|
2,206 |
|
2,088 |
|
888 |
|
|
Net deferred tax asset (liability) |
|
$ |
— |
|
$ |
— |
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
The valuation allowances related primarily to operating loss carry-forwards and temporary differences relating to share-based compensation expense, which management considered are not more likely than not of being realized after weighing all available positive and negative evidence including cumulative losses in recent years and projections of future taxable losses, taxable temporary
F-26
Table of Contents
differences, and prudent and feasible tax-planning strategies.
The valuation allowance increased by $8,182,000 in the year ended December 31, 2016, due to net deferred tax expense related to our continuing operations of $10,107,000, offset by foreign currency translation adjustments of $1,925,000.
Reconciliation of the U.K. statutory income tax rate to the Company’s effective tax rate is as follows (in percentages):
|
|
|
Year ended
December 31,
2016 |
|
Six months ended
December 31,
2015 |
|
Year ended
June 30,
2015 |
|
Year ended
June 30,
2014 |
|
|
|
|
|
|
|
|
|
|
|
|
|
U.K. tax rate |
|
20 |
% |
20 |
% |
20.8 |
% |
22.5 |
% |
|
Permanent differences relating to foreign exchange |
|
— |
|
(8.7 |
)% |
3.4 |
% |
— |
|
|
Surrender of R&D expenditures for R&D tax credit refund |
|
(5.9 |
)% |
(4.5 |
)% |
(5.5 |
)% |
(12.1 |
)% |
|
Change in valuation allowances |
|
(14.7 |
)% |
(10.8 |
)% |
(20.7 |
)% |
(16.2 |
)% |
|
Other |
|
(0.7 |
)% |
4.2 |
% |
0.9 |
% |
5.0 |
% |
|
Effective income tax rate |
|
(1.3 |
)% |
0.2 |
% |
(1.1 |
)% |
(0.8 |
)% |
The Company is headquartered in the United Kingdom and the effective U.K. corporate tax rate for the year ended December 31, 2016, six months ended December 31, 2015 and years ended June 30, 2015 and 2014 was 20%, 20%, 20.75% and 22.5%, respectively. The U.S. federal corporate tax rate was 34% for the year ended December 31, 2016, six months ended December 31, 2015 and years ended June 30, 2015 and 2014.
The United Kingdom’s 2016 Finance Bill, which was enacted on September 15, 2016, contained reductions in corporation tax to 19% from April 1, 2017 and 17% from April 1, 2020. The Company adopted a 17% tax rate at December 31, 2016 in respect of the measurement of deferred taxes arising in the U.K., which reflects the currently enacted tax rate and the anticipated timing of the unwinding of the deferred tax balances. This has reduced from 18% at December 31, 2015. The Company has adopted a 34% tax rate at December 31, 2016 in respect of the measurement of deferred taxes arising in the U.S., which has reduced from 40% at December 31, 2015 due to the U.S. subsidiary being granted an exemption from certain state and local taxes in 2016, which we anticipate being in place for the next several years. The effect of the change in tax rates on the consolidated statement of operations is $nil, after consideration of the change in valuation allowance.
At December 31, 2016, we do not have unremitted earnings in our U.S. subsidiary.
At December 31, 2016, we had U.K. net operating loss and expenditure credit carryforwards of approximately $86.0 million that can be carried forward indefinitely. However, draft legislation has been published in the U.K. for inclusion in the Finance Bill 2017 that would, if enacted, restrict the use of operating loss and expenditure credit carryforwards from April 1, 2017, such that they would not be available for offset against more than 50% of taxable profits in any accounting period (subject to a £5 million annual allowance). We do not have any U.S. net operating loss carryforwards.
Our tax returns are under routine examination in the U.K. and U.S. tax jurisdictions. The scope of these examinations includes, but is not limited to, the review of our taxable presence in a jurisdiction, our deduction of certain items, our claims for research and development credits, our compliance with transfer pricing rules and regulations and the inclusion or exclusion of amounts from our tax returns as filed. The Company is no longer subject to examinations by tax authorities for the tax years 2011 and prior in the U.K. However, U.K. net operating losses from the tax years 2011 and prior would be subject to examination if and when used in a future tax return to offset taxable income. Our U.K. income tax returns have been accepted by Her Majesty’s Revenue and Customs through the period ended December 31, 2015. The Company is subject to examinations by tax authorities in the U.S. for all tax years 2011 through 2016. Our U.S. federal income tax return for the year ended June 30, 2014 was audited by the U.S. Internal Revenue Service and resulted in no changes. We are also subject to audits by U.S. state taxing authorities where we have operations.
Unrecognized tax benefits arise when the estimated benefit recorded in the financial statements differs from the amounts taken or expected to be taken in a tax return because of the uncertainties described above. At December 31, 2016, December 31, 2015 and June 30, 2015 the Company had no unrecognized tax benefits.
F-27
Table of Contents
Note 12 — Geographic information
Operations by geographic area
Revenue represents recognized income from the GSK Collaboration and License agreement. All revenue was derived in the U.K.
Long-lived assets (excluding intangibles and financial instruments) were located as follows (in thousands):
|
|
|
December 31,
2016 |
|
December 31,
2015 |
|
June 30,
2015 |
|
|
|
|
|
|
|
|
|
|
|
U.K. |
|
15,719 |
|
$ |
12,124 |
|
$ |
4,898 |
|
|
U.S. |
|
12,180 |
|
1,101 |
|
494 |
|
|
Total long-lived assets(1) |
|
27,899 |
|
$ |
13,225 |
|
$ |
5,392 |
|
(1) Clinical materials of $2,580,000, $4,736,000 and $nil, included within non-current assets at December 31, 2016, December 31, 2015 and June 30, 2015, are not included within the table above because they can easily be transferred between geographic location.
Major customers:
During the year ended December 31, 2016, six months ended December 31, 2015 and the years ended June 30, 2015 and 2014 revenues were generated from one customer, which was GSK. GSK accounted for 100% of revenue.
F-28